By PAUL HARASIM / RJ
A number of veterans as
well as doctors now
believe that Vietnam
veterans...could have
contracted hepatitis C
through unsafe jet gun
vaccinations.
While it’s possible the government’s position on transmission of hepatitis C among boomers may have resulted in less testing, it’s critical today boomers forget any fears of stigma and get the easy blood test.
Although this issue may be controversial because increased survival has not been demonstrated for this screening practice, a recent consensus conference on the clinical management of hepatocellular carcinoma (4) supported the current widespread practice of performing serum alphafetoprotein levels and liver ultrasound every 6 months. This recommendation was based on available data on tumor growth and with a stated aim of detecting tumors below 3 centimeters (cm) in diameter.
Cirrhosis represents the end stage of any chronic liver disease. Hepatitis C and alcohol are currently the main causes of cirrhosis in the United States. Two major syndromes result from cirrhosis: portal hypertension and hepatic insufficiency. Additionally, peripheral and splanchnic vasodilatation with the resulting hyperdynamic circulatory state is typical of cirrhosis and portal hypertension. In a patient with chronic hepatitis C, a low platelet count (<100,000/mm3) may be indicative of progression to cirrhosis.(1)
Cirrhosis can remain compensated for many years before the development of a decompensating event. Decompensated cirrhosis is marked by the development of any of the following complications: jaundice, variceal hemorrhage, ascites, or encephalopathy. Jaundice results from hepatic insufficiency and, other than liver transplantation, there is no specific therapy for this complication. It is, however, important to recognize and treat superimposed entities (e.g., alcoholic hepatitis, drug hepatotoxicity) that may contribute to the development of jaundice.
The other complications of cirrhosis occur mainly as a consequence of portal hypertension and the hyperdynamic circulation. Gastroesophageal varices result almost solely from portal hypertension, although the hyperdynamic circulation contributes to variceal growth and hemorrhage. Ascites results from sinusoidal hypertension and sodium retention, which is, in turn, secondary to vasodilatation and activation of neurohumoral systems. The hepatorenal syndrome results from severe peripheral vasodilatation that leads to renal vasoconstriction. Hepatic encephalopathy is a consequence of shunting of blood through portosystemic collaterals (as a result of portal hypertension), brain edema (cerebral vasodilatation), and hepatic insufficiency.
The following treatment recommendations for cirrhosis are divided according to the status--compensated or decompensated--of the cirrhotic patient and are based on evidence in the literature, mainly from randomized clinical trials and meta-analyses of these trials, as well as on the results of the most recent consensus conferences. When little or no data exist from well-designed prospective trials, emphasis is given to results from large series and reports from recognized experts. Further controlled clinical studies are needed to clarify aspects of these recommendations, and revision may be necessary as new data appear. Clinical considerations may justify a course of action that differs from these recommendations.
Recommendations are summarized at the end of this document in the Appendix.
II. Management
A. Compensated Cirrhosis
As mentioned previously, patients with compensated cirrhosis are not jaundiced and have not yet developed ascites, encephalopathy, or variceal hemorrhage. Median survival of patients with compensated cirrhosis is around 10 years.(2) At this point in the natural history of cirrhosis, management is essentially preventive and consists of routine monitoring for the development of liver insufficiency and/or the development of complications of portal hypertension/cirrhosis.
Assessments in patients with compensated cirrhosis
The following assessments are recommended:
Liver synthetic function
Screening for gastroesophageal varices
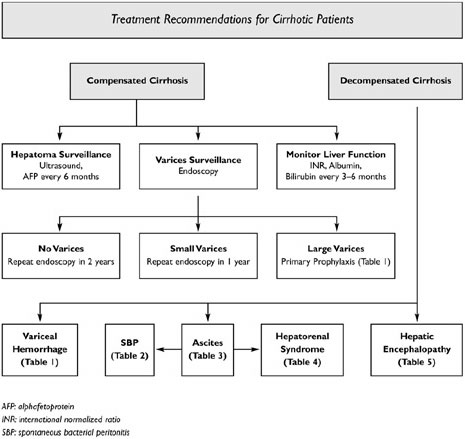
An esophagogastroduodenoscopy (EGD) should be performed once the diagnosis of cirrhosis is established. If no varices are seen, the EGD should be repeated in 2 years. If only small varices are observed, the EGD should be repeated in 1 year and no prophylactic therapy is recommended. If and when the EGD shows large varices, the patient should be started on therapy to prevent the first variceal hemorrhage (see below). These recommendations are based on results of a recent consensus conference on management of portal hypertension and on available data regarding the natural history of varices.(3)
Screening for hepatocellular carcinoma
Although this issue may be controversial because increased survival has not been demonstrated for this screening practice, a recent consensus conference on the clinical management of hepatocellular carcinoma (4) supported the current widespread practice of performing serum alphafetoprotein levels and liver ultrasound every 6 months. This recommendation was based on available data on tumor growth and with a stated aim of detecting tumors below 3 centimeters (cm) in diameter.
Vaccination against hepatitis A and B viruses
As established in the recent National Institutes of Health (NIH) consensus conference on management of chronic hepatitis C (5), all susceptible patients with chronic hepatitis C should be vaccinated against hepatitis A, and seronegative persons with risk factors for hepatitis B should be vaccinated against hepatitis B. This is particularly relevant for patients with cirrhosis in whom a superimposed acute A or B hepatitis could result in decompensation of cirrhosis.
Table 1. Assessments in patients with compensated cirrhosis
The following recommendations are based on expert opinion or formal consensus development processes:
Liver synthetic function tests every 3 to 6 months
EGD
If no varices, repeat endoscopy in 2 years
If small varices, repeat endoscopy in 1 year
If large varices, therapy to prevent first variceal hemorrhage
Alphafetoprotein serum levels and liver ultrasound every 6 months
Vaccination against hepatitis A and B in susceptible individuals
1. Prevention of first variceal hemorrhage
Gastroesophageal varices are present in approximately 50 percent of cirrhotic patients. Their presence correlates with the severity of liver disease; while only 40 percent of Child A patients have varices, they are present in 85 percent of Child C patients.(6) Patients with gastroesophageal varices develop variceal hemorrhage at a rate of around 25 to 30 percent in 2 years. Mortality following variceal hemorrhage is around 30 percent. Therefore, one of the main preventive measures in the compensated cirrhotic is the prevention of first variceal hemorrhage.
Candidates
Three factors identify patients at a high risk of bleeding from varices: large variceal size, red wale markings on the varices, and severe liver failure.(7) Most trials on primary prevention of variceal hemorrhage have included patients with large varices. Patients with small varices have a low risk of bleeding, estimated at 7 percent over 2 years, so specific therapy is not recommended. Patients with gastric varices (with or without esophageal varices) should be treated prophylactically.
Accepted therapy
The results of a meta-analysis of 11 trials evaluating nonselective beta-blockers (i.e., propranolol, nadolol, and timolol) in the prevention of first variceal hemorrhage have been reported recently.(8) Overall, the bleeding rate in controls is 25 percent after a median followup of 24 months and is significantly reduced to 15 percent in beta-blocker-treated patients. Mortality is also lower in the beta-blocker group (23 percent) compared with the control group (27 percent); however, this difference is not statistically significant. This meta-analysis also analyzes the effect of beta-blockers as a function of variceal size.
The risk of first variceal bleeding in patients with large or medium-sized varices is significantly reduced by beta-blockers (30 percent in controls and 14 percent in beta-blocker-treated patients). However, in patients with small varices, the number of patients and the rate of first bleeding were too small to achieve statistical significance. In another meta-analysis based on individual patient data,(9) the beneficial effect of nonselective beta-blockers was present in patients both with and without ascites and in patients with and without poor liver function and was associated with a significant reduction in bleeding-related deaths. Additionally, a cost-effectiveness study comparing nonselective beta-blockers, sclerotherapy, and shunt surgery showed that beta-blockers were the only cost-effective form of prophylactic therapy.(10)
Recommended treatment schedule
The recommended dose of nonselective beta-blockers (propranolol, nadolol, or timolol) is the one that will reduce heart rate to 55-60 beats/minute. Propranolol is given twice a day and is usually started at a dose of 20 milligrams (mg) twice a day (BID). Nadolol and timolol are given once a day (QD). Nadolol is started at a dose of 40 mg QD and timolol at a dose of 10 mg QD. The nonselective beta-blocker on the Department of Veterans Affairs (VA) National Formulary is propranolol (10, 20, 40, and 80 mg tablets).
Based on data from a recent study,(11) it is recommended that prophylactic therapy be continued indefinitely.
Contraindications/side effects
Approximately 15 percent of patients have contraindications to the use of beta-blockers, such as asthma, insulin-dependent diabetes (with episodes of hypoglycemia), and peripheral vascular disease. The most common side effects related to beta-blockers in cirrhosis are lightheadedness, fatigue, and cold extremities.
Some of these side effects disappear with time or after a reduction in the dose of the beta-blocker. Side effects have led around 15 percent of patients to withdraw from clinical trials. The rate of side effects in trials in which nadolol was used (~10 percent) appears to be lower than in trials in which propranolol was used (~17 percent); however, direct comparisons have not been performed.
Alternative therapies
Because endoscopic variceal ligation (EVL) has been shown to be more useful and safe than sclerotherapy in preventing variceal rebleeding, its usefulness in preventing first variceal hemorrhage has also been examined. A meta-analysis comprising 283 patients included in four trials (two published articles, two abstracts) of EVL versus beta-blocker therapy shows that EVL reduced the risk of first hemorrhage from 16 percent in beta-blocker-treated patients to 8 percent in EVL-treated patients with no change in bleeding or overall mortality.(12)
This meta-analysis is largely based on a trial of 90 patients with large varices in which the rate of first variceal hemorrhage was significantly lower in the EVL-treated group (9 percent) compared with the propranolol-treated group (27 percent).(13) However, the rate of first hemorrhage in the propranolol-treated group is unusually high and is comparable to the rate of first hemorrhage in placebo-treated patients, including placebo-treated patients from a prior study by the same group of investigators.(14)
This suggests that patients in the EVL study were not compliant and/or were not adequately beta-blocked. Furthermore, a recent randomized trial, not included in the meta-analysis, showed that EVL was equivalent to propranolol in preventing first variceal bleed.(15) Further studies need to be performed in a larger number of patients before EVL can be widely recommended.
Therapies under investigation
The combination of a nonselective beta-blocker and isosorbide mononitrate (ISMN) has a synergistic portal pressure-reducing effect and could theoretically be more effective than beta-blockers alone in preventing first variceal hemorrhage.(16)
In fact, a nonblinded trial comparing nadolol alone with nadolol plus ISMN demonstrated a significantly lower rate of first hemorrhage in the group treated with combination therapy.(17) These results were maintained after 55 months of followup, without differences in survival.(18) However, two more recent double-blind placebo-controlled trials were unable to confirm these favorable results (19; 20) and a greater number of side effects (mainly headache) were noted in the combination therapy group.(19) Therefore, the use of a combination of a beta-blocker and ISMN cannot be recommended currently for primary prophylaxis until there is further proof of efficacy.
The combination of a nonselective beta-blocker and spironolactone (that has been shown to lower portal pressure by reducing plasma volume and splanchnic blood flow) has been recently examined in a preliminary double-blind placebo-controlled trial.(21) The results suggest that nadolol plus spironolactone does not increase the efficacy of nadolol alone in the prophylaxis of first variceal bleed. However, when bleeding and ascites were considered together, combination therapy significantly reduced the development of either of these complications.
Therapies of proven inefficacy
ISMN alone has been shown in one study to be as effective as propranolol in preventing first variceal hemorrhage.(22) However, long-term followup of patients enrolled in this study showed higher mortality in a subgroup of patients.(23) ISMN, a potent venodilator, may lead to a higher mortality in these patients by aggravating the vasodilatory state of the cirrhotic patient.(24) In a recent multicenter trial, 133 cirrhotic patients with varices and contraindications or intolerance to beta-blockers were randomized to ISMN (n=67) or to placebo (n=66).(25)
Surprisingly, there was a greater 1- and 2-year probability of first variceal hemorrhage in the ISMN group (p=0.056), with no differences in survival. Side effects were more frequent in patients receiving ISMN. These results were further supported in another randomized trial of cirrhotic patients with ascites.(26) Therefore, the use of nitrates alone should be discouraged.
Shunt surgery trials have shown conclusively that, although very effective in preventing first variceal hemorrhage, shunt surgery is accompanied by more frequent encephalopathy and higher mortality.(27) Because the physiology of the transjugular intrahepatic portosystemic shunt (TIPS) is the same as that of surgical shunts (i.e., diversion of blood away from the liver), these results can be extrapolated to TIPS. Therefore, shunt therapy (surgery or TIPS) not only is not recommended but should not be used in the primary prevention of variceal hemorrhage.
Endoscopic sclerotherapy trials have yielded controversial results. While early studies showed promising results, later studies showed no benefit.(27; 28) In fact, a VA prospective randomized cooperative trial comparing prophylactic sclerotherapy and sham therapy had to be terminated 22.5 months after it began, because the mortality rate was significantly higher in the sclerotherapy group than in the sham-therapy group.(29) Sclerotherapy should therefore not be used for the primary prevention of variceal hemorrhage.
Recommendation: Nonselective beta-blockers (propranolol, nadolol, and timolol) are the therapy of choice in patients with medium-sized and large varices that have not yet bled. The dose of beta-blockers should be adjusted to achieve a maximal tolerable decrease in heart rate to a minimum of 55 beats/minute and should be continued indefinitely. Propranolol, the nonselective beta-blocker on the VA National Formulary, should be administered twice a day. Once a patient is on beta-blockers, followup EGD is unnecessary. In patients with contraindications to beta-blockers, or who develop severe side effects and in whom the risk of variceal hemorrhage is very high, EVL should be contemplated. In patients with small varices, the risk of hemorrhage is so small that treatment would not appear to be cost-effective. In these patients, followup EGD should be performed every 1 to 2 years.(3)
Table 2. Primary prophylaxis of variceal hemorrhage in patients with medium or large esophageal varices
The following interventions are recommended based on randomized clinical trials demonstrating delay in time to first variceal hemorrhage:
The following interventions are not recommended based on randomized clinical trials demonstrating that other interventions are either more effective or safer:
Nitrates alone
Endoscopic sclerotherapy
Shunt surgery/TIPS
The following interventions are under evaluation and cannot be recommended until additional information is available:
Combination beta-blocker/nitrates
Combination beta-blocker/diuretics
B. Decompensated Cirrhosis
The following sections deal with the management of the cirrhotic patient who has developed decompensation. Complications are listed in order of severity of the complication and, therefore, in order of their management priority.
1. Treatment of acute variceal hemorrhage
Although bleeding from esophageal varices ceases spontaneously in up to 40 percent of patients, the mortality of an episode of variceal hemorrhage is about 30 percent and occurs mostly in patients with severe liver disease and in those with early rebleeding. Rebleeding occurs in approximately 60 percent of untreated patients within 1 to 2 years of the index hemorrhage.(8) In addition to general measures, the treatment of acute variceal hemorrhage includes the control of hemorrhage (including prevention of early rebleeding) and the prevention of recurrence.
Candidates
Candidates include patients with cirrhosis who present with upper gastrointestinal (GI) hemorrhage and in whom diagnostic endoscopy shows one of the following: active bleeding from a varix, a "white nipple" overlying a varix, clots overlying a varix, or varices with no other potential source of bleeding.(30)
1.a. General measures specific for variceal hemorrhage
A general measure that is currently considered standard in the care of patients with variceal hemorrhage is the use of short-term antibiotic prophylaxis.(31) Cirrhotic patients with upper GI bleeding are at a high risk of developing severe bacterial infections (spontaneous bacterial peritonitis and other infections) associated with early recurrence of variceal hemorrhage and a greater mortality.(32; 33) Although even patients with less severe liver disease (i.e., Child A) are at an increased risk of developing bacterial infections, this risk is highest in those with more severe liver disease (i.e., Child B and C).(34; 35) The use of prophylactic antibiotics in cirrhotic patients with GI hemorrhage has been shown by meta-analysis of controlled clinical trials not only to decrease the rate of bacterial infections but also to increase survival.(36; 37)
Therefore, the use of antibiotic prophylaxis for acute variceal hemorrhage should be considered standard practice in all cirrhotic patients, particularly in those with ascites and more severe liver disease. Antibiotics used in these trials include a combination of orally administered nonabsorbable antibiotics,(38) oral norfloxacin,(39) oral ciprofloxacin,(40) intravenous (i.v.) ofloxacin followed by oral ofloxacin, and i.v. followed by oral amoxicillin clavulanate plus i.v. ciprofloxacin.(34)
The antibiotic schedule recommended by consensus (31) is norfloxacin administered orally at a dose of 400 mg BID for 7 days.(31) The rationale behind the oral administration of norfloxacin, a poorly absorbed quinolone, is the selective elimination of gram-negative bacteria in the gut, minimizing a systemic effect. However, quinolone antibiotics with similar spectrum of activity, such as ciprofloxacin or levofloxacin, could also be recommended. In the majority of patients, administration by mouth or through a nasogastric tube is possible. In cases in which this is not possible, quinolones can be administered intravenously.
Another general measure, which is recommended in the setting of acute variceal hemorrhage, is the cautious transfusion of blood products. Because restitution of lost blood has been shown in experimental animals to lead to increases in portal pressure greater than baseline (41) and to more bleeding,(42) transfusion should aim to maintain the hematocrit between 25 and 30 percent. Intravascular volume overexpansion should also be avoided as this too can precipitate variceal rebleeding.
1.b. Control of acute hemorrhage and prevention of early recurrence
Accepted therapies
Pharmacological therapy has the advantages of being generally applicable and capable of being initiated as soon as a diagnosis of variceal hemorrhage is suspected, even prior to diagnostic EGD. A recent meta-analysis of 15 trials comparing emergency sclerotherapy and pharmacologic treatment (vasopressin alone or in combination with nitroglycerin, terlipressin, somatostatin, or octreotide) suggests that pharmacological therapy should be considered the first-line treatment of variceal bleeding.(43) However, the most effective, safe, and widely accepted drugs are somatostatin and terlipressin, neither of which is available in the United States.
Vasopressin and the somatostatin analogue, octreotide, are available in the United States (and are on the VA formulary). The use of vasopressin is limited by the presence of side effects. Its efficacy and safety are significantly improved by the addition of nitrates.(44) Nevertheless, side effects of combination therapy are still higher than those associated with terlipressin or somatostatin.(8) Vasopressin is administered at a continuous infusion of 0.2--0.4 units/minute, and can be increased to a maximum of 0.8 units/minute. It should always be accompanied by intravenous nitroglycerin at a starting dose of 40 mg/minute that can be increased to a maximum of 400 mg/minute, adjusted to maintain a systolic blood pressure >90 millimeters/hectogram (mm/Hg). Continuous infusion of vasopressin/nitroglycerin cannot be recommended for more than 24 hours because of an increased incidence of adverse effects.
Results of trials of octreotide have been controversial, with two recent meta-analyses showing contradictory results. One of them suggests that octreotide has little or no effect when used alone,(8) while the other shows that octreotide improves control of variceal hemorrhage compared with all alternative therapies.(45) Its side-effect profile was similar to placebo or no therapy; however, it did not show a survival benefit. There are two significant flaws of this meta-analysis.
The first is comparing octreotide to other therapies that are not comparable among themselves (no treatment, vasopressin, glipressin, balloon tamponade, and sclerotherapy). The second flaw is excluding the only double-blind placebo-controlled study of octreotide, which showed that octreotide had no effect.(46) Therefore, the efficacy of octreotide in acute variceal hemorrhage remains unclear. Octreotide is probably not useful as a single first-line therapy of acute variceal hemorrhage, but it may be of use as an adjunct to endoscopic therapy.
Endoscopic therapy is highly effective in controlling active hemorrhage and in preventing early rebleeding and has become the gold standard in the management of acute variceal hemorrhage.(27) However, as mentioned above, a recent meta-analysis of 15 trials comparing sclerotherapy with vasoactive drugs (vasopressin, terlipressin, somatostatin, and octreotide) showed no differences in failure to control bleeding, rebleeding, mortality, or transfused blood units.(43) Another meta-analysis (47) compared sclerotherapy and EVL and concluded that both endoscopic therapies appear equally effective in an emergency. One study that specifically addressed the issue of endoscopic therapy in the control of acute variceal hemorrhage showed in fact that EVL was associated with greater efficacy and fewer complications than sclerotherapy.(48)
Combination of pharmacological therapy and endoscopic therapy appears to be the most promising approach in the treatment of acute variceal hemorrhage. The use of pharmacological agents with few side effects allows prolonging therapy to 5 days, the period during which the risk of rebleeding is the highest. In this way, rather than controlling the acute episode (which is achieved by endoscopic therapy), the goal of pharmacological therapy is the prevention of early rebleeding. A recent meta-analysis of eight trials involving 939 patients showed that combined treatment (vasoactive drugs plus sclerotherapy or EVL) improved the initial control of bleeding and 5-day hemostasis (RR, 1.28; 95 percent CI, 1.18-1.39) without differences in mortality or severe adverse events.(49)
Side effects
Vasopressin is a potent vasoconstrictor with significant side effects related to its vasoconstrictive effect. These include cardiac and peripheral ischemia, arrhythmias, hypertension, and bowel ischemia. As mentioned above, the addition of nitrates reduces the rate of adverse events; however, the combination can only be used continuously for a maximum of 24 to 48 hours to minimize the development of side effects. Octreotide and other somatostatin analogues are safe and can be used continuously for many days (5 days in most trials).
Other therapies
Despite urgent sclerotherapy and/or pharmacological therapy, bleeding cannot be controlled or has an early recurrence in about 10 to 20 percent of patients. Shunt therapy, either shunt surgery (in Child A patients) or TIPS, has proven clinical efficacy as salvage therapy for patients that fail to respond to endoscopic or pharmacological therapy.(50; 51) Although it had been suggested that bleeding from gastric varices was more difficult to control with TIPS than bleeding from esophageal varices, a recent study showed equal effectiveness of TIPS in both situations.(52)
Sclerotherapy is not optimal for patients bleeding from gastric fundal varices. A recent randomized study compared EVL to obliteration with butyl cyanoacrylate in patients actively bleeding from gastric varices.(53) Initial control of hemorrhage, rebleeding rate, treatment-induced ulcers, and survival were all significantly better in patients treated with cyanoacrylate obliteration. Unfortunately, cyanoacrylate is not licensed for use in the United States.
Balloon tamponade is very effective in controlling bleeding temporarily. However, its use is associated with potentially lethal complications and should be limited to patients with uncontrollable bleeding for whom a more definitive therapy (e.g., TIPS) is planned.
Therapies under investigation
Results of ongoing large trials of another somatostatin analogue, lanreotide, should be helpful in establishing the value of somatostatin analogues as adjuncts to endoscopic therapy in the management of acute variceal hemorrhage. Therapies aimed at improving hemostasis (e.g., activated factor VII, antifibrinolytic agents) are ongoing, and results of a recent pilot randomized, placebo-controlled trial using activated recombinant factor VII (rFVIIa) showed a benefit in Child B and C cirrhotic patients.(54)
Recommendation: Short (7-day) antibiotic prophylaxis is recommended in all cirrhotic patients admitted with GI hemorrhage, particularly in those with ascites and a poor liver synthetic function. Although the antibiotic most commonly used in published reports is norfloxacin (not available on the VA National Formulary) administered by mouth (PO) at a dose of 400 mg BID, equal efficacy has been observed with ciprofloxacin at a dose of 500 mg PO BID. This efficacy can most likely be extended to other quinolones, such as levofloxacin.
For patients in whom antibiotics cannot be administered by mouth or by nasogastric tube, quinolones can be administered intravenously. In the United States, endoscopic therapy (either sclerotherapy or EVL) is the therapy of choice in the control of acute variceal hemorrhage. The association of pharmacological therapy, used as soon as the diagnosis is suspected (even prior to endoscopy) and continued for 5 days after the diagnosis is established, may represent the best approach to treatment. Octreotide, the only somatostatin analogue available in the United States, is a reasonable option; however, the efficacy of somatostatin analogues remains to be established definitively in ongoing trials.
The combination of vasopressin plus nitroglycerin is another pharmacological option in the United States, but it can only be used for a maximum of 24 hours. Shunt surgery or TIPS is indicated in patients in whom hemorrhage from esophageal varices cannot be controlled or in whom bleeding recurs in spite of two sessions of endoscopic therapy (associated or not with pharmacological therapy). In patients who bleed from gastric fundal varices, failure of one sclerotherapy session should be enough to recommend shunt therapy. Balloon tamponade should be limited to patients with uncontrollable bleeding for whom a more definitive therapy (e.g., TIPS) is planned.
Table 3. Treatment of acute variceal hemorrhage
The following interventions are recommended based on randomized clinical trials, experimental studies, and meta-analyses
Administration of antibiotic prophylaxis such as norfloxacin (400 mg BID) or ciprofloxacin (500 mg BID)
Conservative blood replacement (goal: hematocrit of 25 to 30 percent)
Early endoscopic diagnosis and therapy (sclerotherapy or EVL)
Early initiation of pharmacological therapy
Octreotide
Vasopressin plus nitroglycerin (for a maximum of 24 hours)
In case of failure to control bleeding or early rebleeding, a prompt decision for rescue therapy should be made (no more than two sessions of endoscopic therapy)
Recommended rescue therapies are TIPS or shunt surgery
The following interventions are not recommended based on randomized clinical trials or uncontrolled studies demonstrating that other interventions are either more effective or safer:
Balloon tamponade should be used only as a bridge to rescue therapy
Emergency surgery or TIPS are not recommended as the first therapeutic option; they are recommended only as rescue therapies
The following interventions are under evaluation and cannot be recommended until additional information is available:
Somatostatin analogues or other pharmacological therapy (use extended to 5 days
Agents to improve hemostasis
1.c. Prevention of recurrent variceal hemorrhage
Patients who survive an episode of acute variceal hemorrhage have a very high risk of rebleeding and death. The median rebleeding rate in untreated individuals is around 60 percent within 1 to 2 years of the index hemorrhage, with a mortality of 33 percent.(8) It is therefore essential that patients who survive an episode of variceal hemorrhage be started on therapy to prevent recurrence prior to discharge from the hospital. Patients who required shunt surgery or TIPS to control the acute episode do not require further preventive measures. However, TIPS occlusion is quite frequent (see below) and reintervention may be necessary if bleeding recurs.
Candidates
Candidates are patients who have recovered from an episode of acute variceal hemorrhage, have had no evidence of hemorrhage for at least 24 hours, and in whom pharmacological therapy for the control of acute variceal hemorrhage has been discontinued.
Accepted therapies
Nonselective beta-blockers and sclerotherapy have reduced variceal rebleeding and death in treated patients compared with untreated controls. In these studies, rebleeding rates of 57 to 63 percent are described in untreated controls compared with rates of 42 to 43 percent in treated patients.(8; 27; 47) A meta-analysis of 10 randomized trials comparing propranolol to sclerotherapy in the prevention of variceal rebleeding shows comparable rates of variceal rebleeding and survival for both therapies, with a significantly higher rate of side effects with sclerotherapy.(8)
Therefore, treatment with nonselective beta-blockers is preferable to sclerotherapy in the prevention of rebleeding. beta-blockers are used at the same doses recommended for prevention of first variceal hemorrhage (see above). As mentioned previously, the combination of a nonselective beta-blocker and ISMN has a synergistic portal pressure-reducing effect and could theoretically be more effective than beta-blockers alone. Only one study has performed a direct comparison between the combination of propranolol plus ISMN and propranolol alone.(55)
This study showed a benefit of combination therapy (33 percent versus 41 percent rebleeding rate), but it was not statistically significant. However, data collected from different randomized clinical trials show lower median rebleeding rates (~33 percent) in patients treated with combined pharmacological therapy compared with rebleeding rates in patients treated with nonselective beta-blockers alone (~50 percent).(8) Therefore, the pharmacological therapy of choice in the prevention of variceal rebleeding is probably the combination of a nonselective beta-blocker and a nitrate.
EVL, compared with sclerotherapy, reduces the rebleeding rate, side effects, and, importantly, mortality.(56) Therefore, EVL is considered the endoscopic treatment of choice in the prevention of variceal rebleeding. EVL sessions are repeated at 7- to 14-day intervals until variceal obliteration, which usually requires two to four sessions. Once eradicated, EGD to evaluate recurrence of varices is usually repeated at 6- to 12-month intervals.
Regarding EVL versus combination pharmacological therapy (beta-blockers plus nitrates), there are three studies showing different results. One study showed a benefit of combination pharmacological therapy,(57) another showed a benefit of EVL,(58) and a third showed no difference among treatment groups, despite a clear tendency in favor of pharmacological therapy.(59) These differences probably reflect the dosage of medications used, patient population, and, ultimately, center expertise.(60) Both therapies would appear to be equivalent. Therefore, the choice between pharmacological therapy and endoscopic therapy will depend on such factors as local expertise, compliance, tolerability, and patient preference.
Contraindications/side effects
The side effects of pharmacological therapy are reportedly more frequent with the combination therapy (beta-blockers plus nitrates) than with beta-blockers alone, mostly in terms of headache and weakness.(8) In fact, in the trial that compared both therapies head-to-head, drug discontinuation because of side effects was significantly greater in the combination therapy group (15 percent versus 2 percent).(55)
In patients that are intolerant to combination therapy, nitrates should be discontinued and beta-blockers alone should be continued. Complications of EVL occur in about 14 percent of cases but are usually minor. The most common complication is transient dysphagia and chest discomfort. Shallow ulcers at the site of each ligation are the rule, but they rarely bleed.
Alternative therapies
Shunt surgery is very effective in preventing rebleeding; however, it markedly increases the risk of hepatic encephalopathy, without an effect on survival.(27; 61) Not surprisingly, recent meta-analyses of 11 trials that compared TIPS to endoscopic therapy show similar results.(62; 63) That is, even though rebleeding is significantly less frequent with TIPS, post-treatment encephalopathy occurs significantly more often after TIPS, without differences in mortality. Additionally, shunt dysfunction occurs quite frequently, with 77 percent of patients requiring balloon angioplasty or re-stenting in the first year.(64) Unfortunately, Duplex sonography is not a sensitive test in predicting the presence of a hemodynamically significant TIPS stenosis. When occlusion is suspected, shunt status should be assessed by venography and direct portal pressure measurements.(65)
Furthermore, a recent trial showed that, even though pharmacological (propranolol plus nitrates) therapy was less effective than TIPS in preventing rebleeding, it caused less encephalopathy, identical survival, and more frequent improvement in Child-Pugh class with lower costs than TIPS.(66) Therefore, TIPS should not be used as a first-line treatment, but as a rescue therapy for patients who have failed pharmacologic plus endoscopic treatment.
Therapies under investigation
Combining endoscopic therapy with pharmacological therapy is rational because non-selective beta-blockers theoretically will protect against rebleeding prior to variceal obliteration and would prevent variceal recurrence. A recent randomized trial demonstrates that the combination of EVL plus nadolol plus sucralfate is more effective in preventing variceal rebleeding than EVL alone,(67) with rebleeding rates of 23 percent and 47 percent, respectively. Currently, it seems reasonable to combine non-selective beta-blockers with ECL in cases where pharmacological therapy or endoscopic therapy have failed.
Therapies that should no longer be used
As mentioned above, EVL has been shown to be superior to sclerotherapy, and has been associated with lower rebleeding rates, a lower frequency of esophageal strictures, and the need for fewer sessions to achieve variceal obliteration.(47; 56) Therefore, sclerotherapy should no longer be considered an adequate therapy to prevent variceal rebleeding.
Trials suggest that EVL is followed by a higher rate of variceal recurrence in comparison with sclerotherapy. Even though meta-analysis shows no significant difference in variceal recurrence between treatments,(47) the efficacy of combination EVL plus sclerotherapy compared with EVL alone in reducing variceal recurrence has been explored. A recent meta-analysis of seven such trials showed that the combination of EVL and sclerotherapy offers no advantage over EVL alone regarding the prevention of rebleeding or reduction of mortality and is associated with a higher complication rate.(68) Therefore, evidence accumulated so far should discourage the use of combination EVL plus sclerotherapy.
Recommendation: Pharmacological therapy with a combination of nonselective beta-blockers and nitrates or endoscopic therapy with EVL are accepted therapies in the prevention of variceal rebleeding. The choice will depend on factors such as expertise, compliance, tolerance, and patient preference. In patients that rebleed on pharmacological therapy or on EVL, the combination of EVL and pharmacological therapy should be considered. TIPS is only indicated in patients in whom rebleeding recurs and in patients treated with combined endoscopic and pharmacologic therapy. In patients who are surgical candidates, shunt surgery can be considered even prior to TIPS in centers where the expertise is available.
Table 4. Prevention of recurrent variceal hemorrhage
The following interventions are recommended based on randomized clinical trials and meta-analyses:
Nonselective beta-blockers (propranolol, nadolol, timolol) plus nitrates
Endoscopic variceal ligation
In case of recurrent variceal bleeding despite the above therapies, pharmacological therapy plus EVL can be recommended
Recommended rescue (third-line) therapies are TIPS or shunt surgery
The following interventions are not recommended based on clinical trials demonstrating that other interventions are either more effective or safer:
Sclerotherapy
EVL plus sclerotherapy
The following intervention is under evaluation and cannot be recommended until additional information is available:
EVL plus pharmacological therapy
2. Treatment of spontaneous bacterial peritonitis (SBP)
SBP is an infection of ascites that occurs in the absence of a contiguous source of infection (e.g., intestinal perforation, intra-abdominal abscess). SBP occurs in 10 to 20 percent of hospitalized cirrhotic patients. When first described, its mortality exceeded 90 percent; however, with early recognition of the disease and prompt and appropriate antibiotic therapy, in-hospital mortality from an episode of SBP has been reduced to around 30 percent. Early diagnosis is a key issue in the management of SBP.
As outlined recently,(31) a diagnostic paracentesis should be performed in any patient admitted to the hospital with cirrhosis and ascites, in any cirrhotic patient who develops compatible symptoms or signs, and in any cirrhotic patient with worsening renal or liver function. The diagnosis is established with an ascites polymorphonuclear count (PMN) of > 250/mm3. Ascites and blood samples for culture should also be obtained as soon as the diagnosis of SBP is suspected as this will aid in the patient's management. In patients with hepatic hydrothorax in whom an infection is suspected and in whom SBP has been ruled out, a diagnostic thoracentesis should be performed.
Spontaneous bacterial empyema, a condition akin to SBP that is defined as a pleural fluid with a PMN count >250/mm3 in a cirrhotic patient, may occur in the absence of ascites or SBP.(69) To increase the sensitivity of the bacteriological culture, ascites and/or pleural fluid should be inoculated at the patient's bedside into blood culture bottles.(31; 70) SBP and spontaneous bacterial empyema should be managed in an identical manner. The following management recommendations in these areas are based on evidence in the literature and are the results of a consensus conference on the diagnosis and management of SBP sponsored by the International Ascites Club.(31)
2.a. Treatment of the acute infection
Accepted therapy
Once an ascites PMN count of >250/mm3 is detected, and before obtaining the results of ascites or blood cultures, antibiotic therapy needs to be started. The antibiotic that has been most widely used in the treatment of SBP is intravenous cefotaxime with which SBP resolves in around 90 percent of treated patients.(71-73)
Other third-generation cephalosporins, such as ceftriaxone, have been shown to be as effective as cefotaxime in uncontrolled studies.(74; 75) In a controlled randomized trial, the combination of amoxicillin and clavulanic acid administered intravenously was shown to be as effective and safe as cefotaxime in the treatment of SBP.(76) Patients who develop SBP on prophylactic quinolones (see below) have responded as well to cefotaxime as patients not on prophylaxis.(77)
Cefotaxime is on the VA National Formulary but may be restricted at the facility or Veterans Integrated Service Network (VISN) level. However, other third-generation cephalosporins with a similar spectrum of activity, such as ceftriaxone, are available and should be equally effective. The intravenous preparation of amoxicillin and clavulanic acid is not available in the United States but another beta-blocam/beta-blocamase inhibitor combination, such as ampicillin/sulbactam, would have a similar spectrum of activity. The susceptibility patterns of individual practice settings should be taken into consideration when selecting the antibiotic for SBP.
Dose and duration
Doses of cefotaxime used in clinical trials have ranged between 2 grams i.v. every 4 hours and 2 grams i.v. every 12 hours. One randomized study compared two different dose schedules of cefotaxime (2 grams every 6 hours versus 2 grams every 12 hours) and showed similar rates of SBP resolution and patient survival with both schedules.(73) Ceftriaxone has been used at a dose of 1 to 2 grams i.v. every 24 hours and ceftazidime at a dose of 1 gram i.v. every 12 to 24 hours. The only study assessing the combination of amoxicillin and clavulanic acid used a dose of 1 gram/0.2 gram i.v. every 8 hours.(76)
Antibiotic treatment can be safely discontinued after the ascites PMN count decreases to below 250/mm3, which was shown to occur in a period of 5 days.(78) Another study shows that 5-day therapy with cefotaxime is as effective as 10-day therapy.(72) Therefore, duration of antibiotic therapy should be for a minimum of 5 days, but given that the median time to SBP resolution in controlled trials is 8 days, this latter duration is probably preferable. A study showed that i.v. ciprofloxacin could be safely switched to oral antibiotics after 2 days of therapy and once a response to therapy is demonstrated by a decrease in ascites PMN.(79)
Side effects
The antibiotics recommended above have been associated with very few side effects and no renal toxicity. Cirrhotic patients have an increased propensity to develop aminoglycoside-induced nephrotoxicity and, therefore, aminoglycosides should be considered as a last resort in the therapy of infections in cirrhotic patients.(80)
Alternative therapies
In patients with community-acquired, uncomplicated SBP (i.e., no renal dysfunction, no encephalopathy), a randomized controlled trial showed that oral ofloxacin (or another fully absorbed quinolone) is a good alternative.(81) Ofloxacin is not on the VA National Formulary, but other quinolones, such as levofloxacin, although not investigated in clinical trials, could be used. These other quinolones would have a theoretical benefit, given a broader coverage of gram-positive organisms, which are increasingly the cause of bacterial infections in cirrhosis.(82; 83) However, the use of quinolones for treatment of SBP will depend on the local prevalence of quinolone-resistant organisms.
Therapies that should not be used.
Cirrhotic patients are particularly prone to develop nephrotoxicity from aminoglycosides and, therefore, their use should be avoided.(80) Because large volume paracentesis (LVP) can be associated with vasodilatation (84) and theoretically can contribute to precipitating renal dysfunction in patients with SBP (who are already predisposed because of the presence of a bacterial infection), the performance of LVP should be delayed until after the resolution of SBP. Likewise, medications that can potentially decrease effective intravascular volume, such as diuretics, should be avoided during acute infection.
Therapies under investigation
Renal impairment, a main cause of death in SBP patients, occurs as a result of a further decrease in effective arterial blood volume that, in turn, probably results from a cytokine-mediated aggravation of vasodilatation. With the objective of determining whether plasma volume expansion can prevent renal impairment, a randomized study comparing cefotaxime and albumin to cefotaxime alone was performed in patients with SBP.(85)
While the rate of infection resolution was the same in both groups, patients who received albumin had significantly lower rates of renal dysfunction (10 percent versus 33 percent), in-hospital mortality (10 percent versus 29 percent), and 3-month mortality (22 percent versus 41 percent) compared with patients who did not receive albumin. The inpatient mortality rate of 10 percent is the lowest described so far for SBP.
The dose of albumin used was arbitrary--1.5 grams per kilogram of body weight (g/kg) during the first 6 hours, followed by 1 g/kg on day 3. The group of patients that appeared to be more likely to benefit from the addition of albumin had a serum bilirubin >4 milligrams/deciliter (mg/dL) and evidence of renal impairment at baseline (blood urea nitrogen [BUN] >30 mg/dL and/or creatinine >1.0 mg/dL). Of note, patients assigned to cefotaxime alone had, at baseline, more renal failure and more liver synthetic dysfunction than those randomized to cefotaxime plus albumin.
Although it is not statistically significant, this suggests that patients in the control group were sicker. Perhaps more important, patients randomized to the control group did not receive albumin even if there was evidence of renal dysfunction at baseline or during followup.
Recommending the use of albumin in every patient with SBP depends on the results of confirmatory studies. These studies will better identify subgroups of patients who will benefit from this adjunctive therapy.
Recommendation: In the presence of an ascites PMN count >250/mm3, intravenous antibiotics should be initiated. The recommended antibiotic is cefotaxime or other third-generation cephalosporins (ceftriaxone, e.g.) or the combination of a beta-blocam/beta-blocamase inhibitor, such as amoxicillin and clavulanic acid. Although cefotaxime is on the VA National Formulary, it may be restricted at the facility or VISN level, in which case ceftriaxone could be used.
The intravenous preparation of amoxicillin and clavulanic acid is not available in the United States and, therefore, the combination of ampicillin/sulbactam could be used instead. In patients with community-acquired SBP, no encephalopathy, and a normal renal function, orally administered quinolones with a high bioavailability are an acceptable alternative, provided that the local prevalence of quinolone-resistant organisms is low.
In patients with renal dysfunction, either at baseline or during treatment, plasma expansion with albumin should be used as an adjunct to therapy. Antibiotic treatment should be administered for a minimum of 5 days, preferably for 8 days. A repeat paracentesis performed 48 hours after starting therapy is generally necessary to assess the response to therapy and the need to modify antibiotic therapy or to initiate investigations to rule out secondary peritonitis. In the presence of an obvious clinical improvement, second paracentesis may not be necessary.
Table 5. Treatment of spontaneous bacterial peritonitis
The following interventions are recommended based on controlled trials or cohort studies demonstrating infection cure rates of around 90 percent:
Intravenous cefotaxime or other third-generation cephalosporins (ceftriaxone) for a duration of 5 to 8 days
Intravenous ampicillin/sulbactam is an alternative
In patients with community-acquired SBP, no renal dysfunction, no encephalopathy, and a low prevalence of quinolone-resistant organisms, an orally administered widely bioavailable quinolone (ofloxacin, levofloxacin) is an alternative
In patients with renal dysfunction, intravenous albumin at a dose of 1.5 g/kg body weight on the first day and 1 g/kg body weight on the third day
The following interventions are not recommended based on clinical trials, uncontrolled studies demonstrating that other interventions are either more effective or safer, as well as theoretical considerations:
Aminoglycoside-containing antibiotic combinations
Procedures and medications that will decrease intravascular effective volume (e.g., large volume paracentesis, diuretics)
The following intervention is under evaluation and cannot be widely recommended until additional information is available:
Intravenous albumin as an adjunct to antibiotic therapy
2.b. Prevention of recurrent SBP
In patients who survive an episode of SBP, the 1-year cumulative recurrence rate is high, at about 70 percent. It is essential, therefore, that patients who survive an episode of SBP be started on antibiotic prophylaxis to prevent recurrence before they are discharged from the hospital.
Accepted therapy
In a double-blind, placebo-controlled study, continuous oral norfloxacin was shown to significantly decrease the 1-year probability of developing recurrent SBP from 68 percent (in the placebo group) to 20 percent (in the norfloxacin group).(86) This was even more obvious for the probability of developing SBP caused by gram-negative organisms, which was reduced from 60 percent to 3 percent.
Prophylactic therapy was discontinued after 6 months of therapy and therefore the effect on survival was not determinable. The median survival of patients who develop SBP is around 9 months (87) and, therefore, antibiotic prophylaxis in this setting does not imply an inordinately prolonged period of administration.
Dose and duration
The dose of norfloxacin used in the abovementioned study was 400 mg by mouth (PO) QD. Prophylaxis should be continued until liver transplantation or the disappearance of ascites (likely to occur in alcoholics who stop alcohol ingestion).
Contraindications/side effects
The development of infections by quinolone-resistant organisms is the main complication of long-term norfloxacin prophylaxis. A recent study, which was performed in a large number of cirrhotic patients hospitalized with an infection, demonstrated that gram-negative bacteria isolated from patients on long-term quinolone prophylaxis were significantly more likely to be not only quinolone-resistant but also trimethoprim/sulfamethoxazole-resistant compared with those of patients not on prophylaxis.(82)
Alternative therapies
Norfloxacin is not on the VA National Formulary; however other quinolones with a similar spectrum, such as ciprofloxacin, could be used instead at a suggested dose of 250 mg QD. Another quinolone, levofloxacin, is also an acceptable substitute with the added advantage of gram-positive coverage. A trial of weekly ciprofloxacin has shown efficacy in the prevention of SBP.(88)
However, the study has methodological problems and, additionally, the use of intermittent ciprofloxacin has been related to a higher occurrence of quinolone-resistant organisms in feces.(89) This higher occurrence was confirmed in a more recent study using weekly rufloxacin in which all 12 patients tested had Escherichia coli resistant to quinolones in their feces by the end of the study.(90) Additionally, this study showed that daily norfloxacin was more effective than weekly rufloxacin in preventing recurrent SBP due to Enterobacteriaceae species.
Therefore, quinolones administered weekly cannot be recommended. Another trial using oral trimethoprim/sulfamethoxazole (one double-strength tablet daily, 5 days per week) (91) also showed efficacy in the prevention of SBP. However, this trial included patients who had had an episode of SBP and patients who had never experienced an episode of SBP, hindering the interpretation of these results. Nevertheless, in patients who are unable to take quinolones, this alternative is reasonable.
Recommendation: Long-term prophylaxis with oral norfloxacin at a dose of 400 mg QD is indicated in patients who have recovered from an episode of SBP. This treatment should be initiated as soon as the course of antibiotics for the acute event is completed. Because norfloxacin is not on the VA National Formulary, oral ciprofloxacin at a dose of 250 mg QD could be used, although levofloxacin may be a better alternative given its added gram-positive coverage. Weekly administration of quinolones is not recommended given a lower efficacy and an increase in the development of fecal quinolone-resistant organisms.(89; 90)
Other antibiotic schedules such as daily trimethoprim/sulfamethoxazole have been insufficiently explored and should not be widely used unless there is further proof of efficacy and only in patients who are intolerant to quinolones (a rare occurrence). Prophylaxis should be continuous until disappearance of ascites (i.e., patients with alcoholic hepatitis who stop drinking) or transplant. As shown below, long-term prophylaxis is currently not recommended in patients with ascites who have never had SBP, regardless of whether refractory ascites and/or a low ascites protein content are present.
Table 6. Prevention of recurrent spontaneous bacterial peritonitis
The following interventions are recommended based on randomized clinical trials or expert opinion:
Oral norfloxacin at a dose of 400 mg QD (not on VA National Formulary)
Oral ciprofloxacin or levofloxacin at a dose of 250 mg QD
The following intervention is not recommended based on clinical trials or uncontrolled studies demonstrating that other interventions are either more effective or safer:
Weekly administration of quinolones
The following intervention is under evaluation and cannot be recommended until additional information is available:
Trimethoprim/sulfamethoxazole
3. Treatment of ascites
Ascites is one of the most frequent complications of cirrhosis. In compensated cirrhotic patients, ascites develops at a 5-year cumulative rate of about 30 percent.(2) Once ascites develops, the 1-year survival rate is around 50 percent compared with 1-year survival greater than 90 percent in patients with compensated cirrhosis.(2; 92-94) Prognosis is particularly poor in patients who develop refractory ascites (95) or hepatorenal syndrome (HRS).(96)
Treatment of ascites has not resulted in significant improvements in survival. However, treating ascites is important, not only because it improves the quality of life of the cirrhotic patient but also because SBP, a lethal complication of cirrhosis, does not occur in the absence of ascites. Most patients have uncomplicated ascites, that is, ascites that is not associated with infection or renal dysfunction and responds to diuretic therapy.(97) Patients go through a sequence of diuretic-responsive ascites, followed by refractory ascites, and then HRS.
3.a. Management of uncomplicated ascites
Candidates
Candidates are cirrhotic patients with ascites not associated with infection or renal dysfunction.(97) Recommendations for uncomplicated cirrhotic ascites apply to patients with uncomplicated hepatic hydrothorax.
Accepted therapy
Sodium restriction is recommended for all cirrhotic patients with ascites. Although dietary sodium should be restricted to levels lower than urinary sodium excretion, sodium restriction to 2 g/day (i.e., 88 milliequivalents per day [mEq/day]) is a realistic goal, particularly in an outpatient setting. Patients with a baseline urinary sodium excretion >50 mEq/day may respond to salt restriction alone. Most patients will require the addition of diuretics.
Spironolactone is the diuretic of choice. Spironolactone can be started alone or in combination with furosemide. It has been shown that spironolactone alone is as effective as combination therapy (spironolactone and furosemide). However, dose adjustments are needed more frequently in the combination group because of the development of increases in blood urea nitrogen and/or decreases in serum sodium.(98; 99) Therefore, it is preferable to initiate therapy with spironolactone alone.
Diuretics can lead to a reduction in intravascular volume and to renal dysfunction and should not be initiated in patients with a rising creatinine level. Additionally, diuretics should not be initiated in patients with concomitant complications of cirrhosis known to be associated with decreased effective arterial blood volume, such as variceal hemorrhage and SBP.
In patients who develop renal dysfunction (elevation in creatinine >50 percent to a creatinine >1.5 g/dL) diuretics should be temporarily discontinued and restarted at a lower dose after creatinine returns to baseline. Patients who develop hyponatremia (serum sodium <130 mEq/L) while on diuretics should be managed with fluid restriction and a decrease in the dose of diuretics.
Dose and duration
The preferred diuretic schedule is to initiate therapy with spironolactone alone at a single daily dose of 100 mg and to increase it in a stepwise fashion to a maximum of 400 mg/day. Because the effect of spironolactone takes several days, it can be administered in a single daily dose and the dose should be adjusted only every 3 to 4 days. If weight loss is not optimal or if hyperkalemia develops, furosemide is then added at an initial single daily dose of 40 mg, increased in a stepwise fashion to a maximum of 160 mg/day. To minimize complications, weight loss in patients without edema should be maintained at a maximum of 1 pound (lb)/day (0.5 kg/day), while a weight loss of 2 lb/day (1 kg/day) is allowable in patients with edema.
Side effects
The more commonly described complications of diuretic therapy are renal impairment due to intravascular volume depletion (25 percent), hyponatremia (28 percent), and hepatic encephalopathy (26 percent).(100; 101; 102) Spironolactone is often associated with adverse events related to its antiandrogenic activity, mainly painful gynecomastia.
Alternative therapies
Potassium canrenoate, one of the major metabolites of spironolactone, has a comparable diuretic effect and a lower antiandrogenic activity and could be used in cases in which gynecomastia and mastalgia are side effects of spironolactone therapy. However, this drug is not available in the United States.
Amiloride, another potassium-sparing diuretic, does not produce gynecomastia and is recommended in patients with intolerable painful gynecomastia, but it has a significantly lower natriuretic effect than spironolactone.(103) Amiloride is used at an initial dose of 20 mg/day and can be increased to 60 mg/day. For patients whose natriuretic response on amiloride is suboptimal it may be worthwhile to attempt retreatment with spironolactone.
LVP, plus intravenous albumin, has been shown to be as effective as standard therapy with diuretics but with a significantly faster resolution and the same or a lower rate of complications.(100; 101; 104) Because this therapy is significantly more expensive and requires more resources than the administration of diuretics, it is reserved for patients not responding to diuretics (see below).
However, in hospitalized patients with moderate to tense ascites in whom other complications have been resolved, it is reasonable to initiate therapy with total paracentesis with concomitant albumin infusion followed by the administration of diuretics. This therapy will accelerate the patient's discharge from the hospital.
Therapies that should not be used
Diuretics. Two randomized trials have shown significantly lower efficacy of the loop diuretic furosemide used alone compared with spironolactone alone (98; 105) or with the combination spironolactone/furosemide.(98) When furosemide is used alone, sodium that is not reabsorbed in the loop of Henle is taken up at the distal and collecting tubules because of the hyperaldosteronism present in most cirrhotic patients with ascites. Therefore, furosemide should not be used as the sole agent in the treatment of cirrhotic ascites.
Nonsteroidal anti-inflammatory drugs or aspirin. These drugs blunt the natriuretic effect of diuretics and therefore should not be used in cirrhotic patients with ascites.(106; 107) Cyclooxygenase-2 inhibitors may also be detrimental and their use should be avoided until additional clinical data are available.
Antibiotic prophylaxis. As mentioned above, short-term antibiotic prophylaxis is recommended in cirrhotic patients (with or without ascites) admitted with GI hemorrhage. Long-term prophylactic antibiotics are recommended in patients with ascites who have recovered from an episode of SBP. However, there are insufficient data to support the use of long-term antibiotic prophylaxis in cirrhotic patients with ascites who are not bleeding and who have not had a previous episode of SBP.
In the only placebo-controlled trial of primary prophylaxis of SBP in patients with low-protein ascites, rates of SBP were low and not significantly different between patients treated with norfloxacin (0 percent) and those treated with placebo (9 percent).(108) On the other hand, long-term antibiotic prophylaxis has led to a significant increase in infections due to quinolone-resistant organisms in patients with cirrhosis.(82) Therefore, until future trials identify a higher-risk population in whom SBP can be prevented with antibiotic therapy, long-term antibiotic primary prophylaxis of SBP is not recommended.
Therapies under investigation
A recent double-blind crossover study suggests that the estrogen antagonist tamoxifen at a dose of 20 mg BID may be useful in the management of painful gynecomastia in cirrhotic patients.(109) This needs further investigation.
Recommendation: Patients with new onset ascites and normal renal function, in whom SBP has been ruled out, should receive treatment with sodium restriction and/or diuretics. Patients with a small amount of ascites and a reasonable urinary sodium excretion (>50 mEq/day) can be started on salt restriction alone. Patients with moderate/tense ascites and avid sodium retention should be treated with sodium restriction and diuretics.
In patients who decrease food intake because of the nonpalatable salt-restricted diet, it is preferable to liberalize sodium intake and implement measures to increase sodium excretion through the use of diuretics, rather than to compromise nutrition. The preferred diuretic schedule is to initiate therapy with spironolactone alone at a single daily dose of 100 mg and to increase it in a stepwise fashion to a maximum of 400 mg/day.
If weight loss is not optimal or if hyperkalemia develops, furosemide is then added at an initial single daily dose of 40 mg, increased in a stepwise fashion to a maximum of 160 mg/day. To minimize the rate of complications, weight loss in patients without edema should be maintained at a maximum of 1 lb/day (0.5 kg/day), while a weight loss of 2 lb/day (1 kg/day) is allowable in patients with edema.
In a hospitalized patient with moderate/tense ascites in whom other complications have been resolved, it is reasonable to initiate therapy with total paracentesis with concomitant albumin infusion followed by the administration of diuretics, as this will accelerate discharge from the hospital. Serial monitoring of urinary sodium is unnecessary in patients who are responding adequately to diuretics, as assessed by daily weights.
Table 7. Treatment of uncomplicated ascites
The following interventions are recommended based on controlled and uncontrolled studies as well as expert opinion:
Salt restriction
Spironolactone plus furosemide
Large-volume paracentesis plus albumin in hospitalized patients with tense ascites in whom other complications have been resolved
Short-term (7-day) antibiotic prophylaxis in cirrhotic patients with (or without) ascites admitted with GI hemorrhage
The following interventions are not recommended, based on clinical trials demonstrating that other measures are either more effective or safe:
Furosemide alone
Long-term antibiotic prophylaxis
3.b. Treatment of refractory ascites
Refractory ascites, present in 10 to 20 percent of cirrhotic patients with ascites, assumes either diuretic-resistant ascites (ascites that is not eliminated even with maximal diuretic therapy) or diuretic-intractable ascites (ascites that is not eliminated because maximal doses of diuretics cannot be attained given the development of diuretic-induced complications such as hepatic encephalopathy, renal abnormalities, and/or electrolyte abnormalities).(110)
However, before making the diagnosis of refractory ascites, it is necessary to ascertain whether the patient has adhered to the prescribed sodium-restricted diet and has refrained from using nonsteroidal anti-inflammatory drugs, which blunt the response to diuretics. Nonadherence to dietary sodium restriction and/or diuretics should be suspected if patients fail to lose weight despite an adequate 24-hour urine sodium excretion (>50 mEq/L or greater than daily sodium intake).
Candidates
Candidates are cirrhotic patients with ascites who fail to respond to diuretics (despite adherence to diet and drugs) or who present complications that preclude the administration of adequate doses of these drugs. Recommendations for patients with refractory ascites apply to patients with refractory hepatic hydrothorax, although these patients should undergo in-hospital careful diuretic therapy before the hydrothorax is considered refractory.
Accepted therapy
Currently, LVP plus albumin is the standard therapy for refractory ascites. In all LVP studies, diuretics are discontinued before and restarted after the procedure. The need to discontinue diuretics prior to LVP has not been well analyzed and, in practice, it is not performed routinely. A trial has shown that the administration of diuretics after LVP is associated with less-frequent recurrence of ascites without any differences in complications. Therefore, sodium restriction and diuretics at the maximal tolerated dose should be used in conjunction with serial LVP.
The need for concomitant administration of intravenous albumin was demonstrated in two trials. The first showed that daily LVP without intravenous albumin is associated with a significantly higher incidence of hyponatremia and renal impairment than LVP with albumin.(111) In another trial, albumin was shown to be associated with a lower incidence of post-paracentesis circulatory dysfunction (PCD) (18 percent) compared with synthetic plasma expanders (38 percent for polygeline and 34 percent for dextran-70).(112) PCD is defined as an increase in plasma renin activity on the sixth day after paracentesis (indicating a decreased effective arterial blood volume). PCD is associated with faster reaccumulation of ascites and a significantly shorter median survival time (10 months versus 17 months).
Recommended treatment schedule
Because LVP is a local therapy that does not act on any of the mechanisms that lead to the formation of ascites, recurrence of ascites is the rule rather than the exception. The frequency of LVPs is determined by the rate of ascites reaccumulation and, ultimately, by the need to relieve the patient's discomfort. In turn, the rate of ascites reaccumulation depends largely on the patient's compliance with salt restriction and use of diuretics.
Albumin should be administered at a dose of 6-8 g of albumin i.v. per liter of ascites extracted. For paracentesis of less than 5 L, a synthetic plasma expander (Haemaccel® dextran-70) can be used instead of albumin, and it has been suggested that no plasma expansion may be necessary in this setting.(97; 112)
Contraindications/side effects
As mentioned above, a complication of LVP, particularly without the concomitant administration of albumin, is PCD, which is characterized by a significant increase in plasma renin activity after paracentesis. PCD appears to be secondary to a worsening in the vasodilatory state.(84) Therefore, LVP should not be performed when there is a worsening in the vasodilatory state of cirrhosis, such as SBP.
Alternative therapies
TIPS is considered a second-line therapy for refractory ascites. This recommendation is based mostly on the results of two recent large multicenter studies comparing LVP plus albumin to TIPS.(113; 114) Although, as expected, recurrence of ascites after LVP was significantly greater in patients randomized to LVP plus albumin, there were no differences in mortality. There was, however, a higher rate of severe encephalopathy and a higher cost in the group randomized to TIPS. Therefore, TIPS should be relegated to a secondary position in the treatment of refractory ascites and is mainly indicated in patients who require LVP frequently--that is, three or more LVP/month.(97)
Peritoneo-venous shunting (PVS) is an alternative to LVP plus albumin. In two randomized trials comparing LVP plus albumin to PVS, both procedures were shown to be equally effective, to have a similar rate of complications, and to have a comparable survival rate.(111; 115) Because of its high obstruction rate, PVS required longer admissions for shunt revision or for the management of other more serious complications. The use of PVS has been practically abandoned because LVP plus albumin is a simpler procedure that can be performed in an outpatient setting. Additionally, the placement of a PVS may hinder the future placement of TIPS and may complicate liver transplant surgery given its ability to produce peritoneal adhesions. Therefore, PVS is mostly indicated in patients who require LVP frequently and who are not candidates for TIPS or for transplant.
Therapies that should not be used
As mentioned above, long-term prophylaxis with norfloxacin is recommended in patients with ascites who have recovered from an episode of SBP. Currently, there is insufficient data to support the use of long-term antibiotic prophylaxis in cirrhotic patients with ascites who are not bleeding and who have not had a previous episode of SBP. In patients with refractory hepatic hydrothorax, the insertion of a chest tube should be proscribed as this will lead to massive fluid losses, a further depletion of the intravascular effective volume, and to renal dysfunction.
Recommendation: Repeated large volume paracenteses plus intravenous albumin is the first-line therapy for refractory ascites. Albumin is infused at a dose of 6-8 g/L of ascites removed. In patients from whom <5 L is being removed, synthetic plasma expanders can be used instead of albumin, and it has been suggested that plasma volume expansion may not be necessary in this situation. Sodium restriction and diuretics should be used concomitantly with LVP. TIPS should be relegated to patients with refractory ascites who require very frequent sessions of LVP and in whom a favorable post-TIPS evolution can be predicted (i.e., patients with a Child-Pugh score of <12 points). PVS should be relegated to patients with refractory ascites who require very frequent sessions of LVP and who are not candidates for TIPS or transplant.
Table 8. Treatment of refractory ascites
The following interventions are recommended based on randomized controlled studies:
LVP plus albumin, associated with salt restriction and diuretics
In patients in whom <5 L is extracted, a synthetic plasma volume expander may be used instead of albumin or plasma volume expansion may not be necessary
In patients requiring frequent LVP, TIPS is an option
In patients requiring frequent LVP, who are not TIPS or transplant candidates, PVS is an option
The following intervention is not recommended based on controlled clinical trials demonstrating that other interventions are either more effective or safer:
PVS or TIPS a s first-line therapy
3.c. Treatment of HRS
HRS is considered part of the clinical spectrum of the cirrhotic patient with ascites. It represents the result of extreme vasodilatation with an extreme decrease in effective blood volume, which leads to maximal activation of vasoconstrictive systems, renal vasoconstriction, and renal failure. HRS has been divided into type 1 and type 2.(110; 116) Patients who develop HRS generally have very poor liver function, and improving renal function probably will not have a major impact on survival. However, with the availability of liver transplant, particularly from living related donors, a small increase in survival may give patients time to obtain a transplant and thereby increase their long-term survival.
Candidates
Type 1 HRS is characterized by rapidly progressive renal failure with a doubling of serum creatinine to a level greater than 2.5 mg/dL or a halving of creatinine clearance to less than 20 milliliters/minute (ml/min) in less than 2 weeks. The prognosis of type 1 HRS is extremely poor, with a median survival of about 2 weeks.(96) In type 2 HRS, serum creatinine is greater than 1.5 mg/dL and/or creatinine clearance is less than 40 ml/min, but renal failure progresses more slowly and there is a better prognosis.
Accepted therapy
The first choice therapy for HRS is liver transplantation. Patients with type 2 HRS have a longer survival rate and this improves their chances to obtain a liver transplant. This is not the case for patients with type 1 HRS whose very short survival rate makes the feasibility of liver transplantation very unlikely, unless survival can be increased by short-term temporizing measures. These are the measures that are under investigation and that have, in uncontrolled studies, been shown to improve renal function and to prolong survival slightly.
Therapies under investigation
In small studies, prolonged (15-day) use of arteriolar vasoconstrictors--such as ornipressin,(117; 118) terlipressin,(119) or the combination of octreotide plus midodrine (120) together with volume expansion with albumin--has shown promise in the treatment of type 1 HRS. However, controlled studies involving larger numbers of patients are required before this treatment can be widely recommended.
More recently, the combination of intravenous noradrenaline (at a dose of 0.5-3 mg/hour) in combination with intravenous albumin given for 10 days was shown to reverse HRS in 10 of 12 patients.(121) It is notable that in many patients this therapy has been discontinued without recurrence of HRS, suggesting that these patients experience either an improvement in liver status (as would occur in alcoholic liver disease with abstinence) or the resolution of a transient decompensating factor such as infection.
Small uncontrolled studies also suggest that TIPS may be useful in the treatment of type 1 HRS and type 2 HRS.(122; 123) More recently, a prospective controlled trial using the molecular adsorbent recirculating system (MARS), a modified dialysis method using an albumin-containing dialysate, was shown to improve 30-day survival in eight patients with HRS compared with five untreated controls.(124) Larger controlled trials are required before the use of TIPS or MARS can be recommended.
Therapies of proven inefficacy
Renal venodilators, such as prostaglandins and dopamine (at nonpressor doses), have been used in patients with HRS in an attempt to reduce intrarenal vascular resistance, without an obvious benefit.(125-129) The combination of peripheral vasoconstrictors plus renal vasodilators has also failed to improve renal function in patients with HRS.(130)
A recent trial compared the effects of octreotide infusion (50 mg/hour) plus albumin with placebo using a randomized, double-blind, crossover design.(131) After 4 days of continuous infusion (octreotide or placebo) plus albumin there was no improvement in renal function, urinary sodium, or plasma renin activity, leading to the conclusion that octreotide alone is not effective for the treatment of HRS in cirrhotic patients.
Recommendation: Liver transplantation is likely to remain the definitive treatment for HRS in patients with cirrhosis. Vasoconstrictors together with plasma volume expansion or TIPS may act as a bridge to transplantation for these patients, but this remains to be determined.
Table 9. Treatment of hepatorenal syndrome
The following intervention is the recommended (definitive) therapy based on expert opinion:
Liver transplant
The following interventions are not recommended based on clinical trials demonstrating a lack of benefit compared to no therapy or placebo therapy:
Octreotide alone
Prostaglandins
Dopamine
Dialysis
The following interventions are under evaluation and cannot be recommended until additional information is available:
Systemic vasoconstrictors plus albumin
TIPS
MARS
4. Treatment of hepatic encephalopathy (HE)
As recently defined in a consensus conference,(132) HE reflects a spectrum of neuropsychiatric and psychometric test performance abnormalities occurring in patients with significant liver dysfunction after exclusion of other known brain diseases. HE, therefore, represents a continuum from minimal (formerly called subclinical) to different degrees of severity of overt HE. Hepatitis C has been associated with neuropsychiatric disturbances that appear to be pathogenetically different from HE. This difference should be taken into account when evaluating a patient with hepatitis C.
The above consensus statement identified the need for therapeutic trials based on different types and clinical settings of HE (e.g., episodic HE, persistent HE, minimal HE, etc.). Because the development of HE per se is not lethal, management recommendations refer essentially to the treatment of overt HE rather than to its prophylaxis. However, HE can be prevented by limiting the use of a common precipitant of HE: sedatives such as benzodiazepines.
In general, the goals of treatment include identification and correction of precipitating factors, as well as measures aimed at reducing the brain concentration of ammonia.(133)
Accepted therapy
Perhaps the most important facts to be recognized are that (1) HE is reversible and (2) a precipitant cause can be identified in the majority of patients.
In a study of 100 cases, HE was precipitated in 80 percent of the cases by factors such as GI hemorrhage, increased protein intake, infection (including SBP), prerenal azotemia, hypokalemic alkalosis, constipation, hypoxia, or the use of sedatives and tranquilizers.(134) The mainstay in the treatment of HE is the identification and treatment of the precipitant cause.
Ammonia has been consistently identified as an important factor in the pathogenesis of HE. Ammonia is largely derived from the GI tract by urease activity of bacteria in the colon and by deamination of glutamine in the small bowel. Reduction of ammonia load can be achieved by acidifying the contents of the colonic lumen, by cleansing the bowel, and by the use of antibiotics.
Lactulose is a nonabsorbable disaccharide that reduces ammonia by acidifying the colon and reducing colonic transit time. It has become the standard drug in the treatment of HE given its good safety profile and large clinical experience, even though the evidence from clinical trials is not conclusive. The route of administration is ideally by mouth. Lactulose enemas should be administered in patients who are unable to take it by mouth. Acidifying enemas have been shown to be superior to tap-water enemas.(135)
Dose and duration
In acute episodic HE, lactulose should be given initially at a large dose (50 ml) every 1 to 2 hours until a bowel movement occurs. After catharsis begins, the oral dose should be adjusted to obtain two to three soft bowel movements/day (15--30 ml BID).
Lactulose enemas (300 mL in 1 L of water) should be given every 6 to 8 hours until the patient is awake enough to start oral intake. In chronic HE (persistent HE), treatment is with oral lactulose adjusted to obtain two to three soft bowel movements/day with a starting dose of 30 ml BID. An initial loading dose is not necessary. In either case, care should be taken to avoid diarrhea, because the resulting dehydration and electrolyte abnormalities can worsen HE and lead to renal dysfunction.
Side effects
The common side effects of lactulose therapy include unpleasant taste, bloating, abdominal cramps, and diarrhea. If diarrhea develops, lactulose should be withheld until diarrhea resolves and then restarted at a lower dose. It is important to note that the presence of diarrhea in a cirrhotic patient can be more detrimental than HE itself, as it can reduce the effective arterial volume and, therefore, can potentially lead to renal deterioration.
Alternative therapies
Antibiotics achieve reduction of ammonia load by elimination of colonic bacteria. Neomycin, a poorly absorbed aminoglycoside, has been utilized in the treatment of HE, combined with sorbitol or milk of magnesia (to accelerate intestinal transit and to cleanse the bowel), and has been shown to be as effective as lactulose.(136) However, long-term use may produce nephrotoxicity and ototoxicity. In another small clinical trial, metronidazole at a dose of 200 mg QID was shown to be as effective as neomycin 1 g QID.(137) However, chronic use of metronidazole may cause side effects such as peripheral neuropathy.
Therefore, the use of antibiotics in HE should be restricted to patients who have not responded to the previously mentioned measures or in whom HE recurs frequently. Persistent and intractable post-TIPS HE can be treated by occluding the shunt or reducing its diameter.
Adjunctive therapy
A protein and energy malnutrition state is common in patients with cirrhosis. One common mistake in HE management is inappropriate and prolonged protein restriction, particularly considering that cirrhosis is a catabolic state with a higher daily protein requirement than normal. In acute HE, short-term (2 to 3 days) protein restriction may be useful.
However, prolonged restriction will result in malnutrition, which may worsen the prognosis of cirrhotic patients.(138) Suggested protein intake in cirrhotics (with or without HE) is 1--1.5 g/kg/day. It has been suggested that protein from vegetables and dairy products gives a higher calorie per nitrogen ratio and hence produces less ammonia than animal protein.(139) The role of branched-chain amino acid supplements in the treatment of chronic HE is not yet established and could be proposed for patients who are intolerant of alimentary proteins.(140)
Therapies that should not be used
For the reasons stated above, long-term protein restriction should be avoided. It is important to note that cirrhotic patients are highly susceptible to the sedative effect of benzodiazepines and doses considered therapeutic are able to precipitate prolonged coma or near-coma.
Therefore, benzodiazepines and other sedative drugs (antihistamines, narcotics, and antidepressants with sedative effects) should be avoided or administered very carefully and at lower doses in cirrhotic patients.
Eradication of Helicobacter pylori, a urease-producing bacteria found in the upper GI tract, has not been shown to be helpful in the treatment of HE.(141)
Therapies under investigation
Various therapies directed at reversing alterations of various neurotransmitters postulated in pathogenesis of HE--such as bromocriptine and flumazenil, or in the urea cycle, such as ornithine aspartate and benzoate--have been investigated and shown in limited trials to be useful in the treatment of HE.(133)
Regarding flumazenil, a benzodiazepine receptor antagonist, two recent meta-analyses show a beneficial effect on HE. One of them showed a significant clinical and electroencephalographic improvement of HE in patients treated with flumazenil from 5 minutes to 3 days.(142) The other showed that, while flumazenil had no significant effect on recovery or survival from HE, it was associated with a significant improvement in HE at the end of treatment.(143)
Considering the fluctuating nature of HE, future trials should use a parallel design and should assess whether treatment with flumazenil leads to a sustained improvement in HE or to increased recovery and survival. Until this has been demonstrated, flumazenil may be considered for patients with chronic liver disease and HE, but it cannot be recommended for routine clinical use.
Recommendation: The initial management of acute, episodic HE involves two steps. The first step is the identification and correction of precipitating causes. Careful evaluation should be performed to determine the presence of hypovolemia, gastrointestinal bleeding, infections (including SBP), and intake of sedatives or tranquilizers. The second step is the administration of lactulose (orally or by enema). Patients with chronic HE should be treated with oral lactulose at a dose adjusted to obtain two to three soft bowel movements/day. In patients with chronic HE who are not tolerant or do not respond to lactulose, the addition of neomycin (starting at 1-3 g per day in three doses) or metronidazole (starting at 250 mg PO BID) may be of benefit. Long-term protein restriction should be avoided and a protein content of 1-1.5 g/kg/day protein diet is recommended. Protein from dairy or vegetable sources may be preferable to animal-derived protein.
Table 10. Treatment of Hepatic Encephalotherapy
The following interventions are recommended based on clinical trials and expert opinion:
Identification and treatment of precipitating event
Short-term protein restriction
Lactulose by mouth or through nasogastric tube, adjusted to two to three bowel movements/day
Lactulose enemas in patients who are unable to take it by mouth
In patients with chronic HE who cannot tolerate lactulose or do not respond to lactulose, treatment with laxatives plus neomycin can be considered
The following intervention is not recommended based on expert opinion:
Long-term protein restriction
The following interventions are under evaluation and cannot be recommended until additional information is available:
Maximal tolerable dose to reduce heart rate to 55-60 beats/minute
Acute Variceal Hemorrhage
Upper GI hemorrhage with the following endoscopic findings:
Active bleeding from a varix or
Stigmata of variceal bleeding or
Presence of gastro-esophageal varices without other sources of bleeding
First-line therapy
Endoscopic therapy (sclerotherapy or band ligation) ± drug therapy
Short-term antibiotic prophylaxis (see Table 2)
Rescue therapy
Shunt surgery or TIPS
Not recommended
Balloon tamponade (except as a bridge to rescue therapy)
An additional benefit may be derived by associating endoscopic therapy with drug therapy (see text)
Cautious transfusion of fluid and blood products is recommended (goal hematocrit 25 to 30 percent)
Secondary Prophylaxis
Prior history of variceal hemorrhage (with hemo-dynamic stability for 24 hours)
First-line therapy
Nonselective beta-blockers + nitrates
Alternative therapy
Endoscopic variceal band ligation
Rescue therapy
Shunt surgery or TIPS
Not recommended
Sclerotherapy
In patients intolerant to combination pharmacological therapy, treat with beta-blockers alone
In patients who failed pharmacological therapy or ligation, a combination of both can be considered
Table A-2. Recommended management of spontaneous bacterial peritonitis (SBP)
Treatment Type
Recommendations
Comment
Primary Prophylaxis
Long-term prophylaxis not recommended, regardless of ascites protein levels
Short-term (7-day) prophylaxis with a quinolone (norfloxacin, ciprofloxacin, or levofloxacin) is recommended in patients admitted with GI hemorrhage
Short-term antibiotic prophylaxis should be performed independent of the presence or absence of ascites, although patients with ascites and severe liver disease are the ones most likely to benefit
Active Spontaneous Bacterial Peritonitis
Recommended therapy
Intravenous cefotaxime or other third-generation cephalosporin (ceftriaxone)
Intravenous ampicillin/sulbactam
Alternative therapy
Oral ofloxacin or other fully absorbed quinolones (levofloxacin) (depending on prevalence of quinolone-resistant organisms at each institution)
Adjunctive therapy
Intravenous albumin in selected patients
Not recommended
Aminoglycosides
Recommended duration of treatment is 8 days
In case of no obvious improvement despite antibiotics, a followup paracentesis at 48 hours is recommended
Oral therapy may be considered in community-acquired SBP in the absence of renal dysfunction and encephalopathy
Albumin is recommended in patients with renal dysfunction and hyperbilirubinemia (bilirubin >4 mg/dL) at time of SBP diagnosis
Avoid interventions that may further decrease intravascular volume (e.g. large volume paracentesis, diuretics)
Trimethoprim-sulfamethoxazole onedouble-strength tab PO every day
Not recommended
Weekly ciprofloxacin
Prophylaxis should be given until the disappearance of ascites, time of transplantation, or death
Patients who develop quinolone-resistant organism may also have resistance to trimethoprim-sulfamethoxazole
Table A-3. Recommended management of ascites
Ascites Type
Recommendations
Comment
Uncomplicated Ascites
Recommended therapy
Sodium (salt) restriction +/-
Diuretics (spironolactone +/- furosemide)
Initial LVP plus albumin infusion in hospitalized patients with moderate or tense ascites
Recommended sodium restriction of no less than 2 g/day
Dose of diuretics: spironolactone 100-400 mg/day, furosemide 40-160 mg/day
Dose of albumin 6-8 g/L of ascites removed
Amiloride may be used in patients who do not tolerate spironolactone
Adjustment in diuretic dosage should be performed every 4-7 days
Not recommended
Furosemide alone
NSAID use should be avoided
Refractory Ascites
Recommended therapy
LVP plus albumin (continue with salt restriction and diuretic therapy as tolerated)
If less than 5 liters of ascites is extracted, a synthetic plasma volume expander may be used instead of albumin or may not be necessary particularly in patients with normal renal function
Alternative therapy
TIPS in patients who require frequent LVP
PVS in patients who are not TIPS or transplant candidates
Not recommended
TIPS or PVS as first-line therapy
Table A-4. Recommended management of hepatorenal syndrome
Treatment of Hepatorenal Syndrome (HRS)
Recommended Therapy
Liver transplantation
Rescue Therapy (as a bridge to transplantation)
These therapies are still considered experimental
Albumin plus vasoconstrictors: midodrine plus octreotide, norepinephrine, ornipressin, or terlipressin (last two not available in the U.S.)
Table A-5. Recommended treatment of hepatic encephalopathy (HE)
Treatment Type
Recommendations
Comment
General Measures
Identification and treatment of the precipitating cause(s)
Avoidance of sedatives and tranquilizers
Nutritional support
Protein from dairy or vegetable sources are preferable to animal protein
Acute Hepatic Encephalopathy
Recommended therapy
Lactulose 45 cc PO every hour until bowel evacuation then adjust to a dose that will result in two to three bowel movements/day (usually 15-30 cc PO BID)
Alternative therapy
Neomycin 3-6 g PO every day in three doses plus milk of magnesia
Metronidazole starting at 250 mg PO BID
Lactulose enemas (300 cc in 1 liter of water) in patients who are unable to take it by mouth.
Short-term (<72 hours) protein restriction may be considered in severe HE
Chronic Hepatic Encephalopathy
Recommended therapy
Lactulose dosage that produces two to three bowel movements/day, starting at 15-30 cc PO BID
Alternative therapy
Neomycin starting at 1-3 g PO QD (three divided doses)
Metronidazole starting at 250 mg PO BID
Not recommended
Long-term protein restriction
Helicobacter pylori eradication
Patients on chronic antibiotics need to be monitored for nephrotoxicity, ototoxicity, and neurotoxicity
Protein from dairy or vegetable sources may be preferable to animal protein
VA National Hepatitis C Program of the Public Health Strategic Health Care Group: Michael Rigsby, MD (director), Jane Burgess, ACRN, MS, Victoria Davey, RN, MPH, Connie Raab, and Lawrence R. Deyton, MSPH, MD (chief consultant); and VA Hepatitis C Resource Centers: Guadalupe Garcia-Tsao, MD, Suchat Wongcharatrawee,MD, Teresa L.Wright, MD, Samuel B. Ho, MD, and Jason A. Dominitz, MD, MHS; as well as the VA Hepatitis C Technical Advisory Group: Garth Austin, MD, PhD, Joseph Awad, MD, Edmund Bini, MD, FACP, FACG, Lynn Bradley, PA, Robert Dufour,MD, Judith Feldman, MD, MPH, Katherine P. Frandsen, RN, CIC, Curt Hagedorn, MD, Rhonda Jankovich, RN, BSN, Karen Jones, Linda Jones, MSN-RN, Stephen Kendall, Daniel Kivlahan, PhD, Kathy Lockhart, RN, MSN, MPA,Thomas Mahl, MD, Robert McNamara, Shvawn McPherson-Baker, PhD,Timothy Morgan, MD, Linda Rabeneck, MD, David Rimland, MD, Gary Roselle,MD, Hugo Rosen, MD, Kimberly Summers, PhD, and Michael Valentino, RPh.
Dr. Garcia-Tsao and Dr. Wongcharatrawee are the lead authors of this document.
About VA Programs in Hepatitis C
The Department of Veterans Affairs (VA) leads the country in hepatitis C screening, testing, treatment, research and prevention. VA is the largest single provider of medical care to people with hepatitis C infection in the United States.
The National Hepatitis C Program works to ensure that veterans with or at risk for hepatitis C receive the highest quality health care services from the VA system. Led by the VA's Public Health Strategic Healthcare Group (PHSHG) and carried out by VA medical facilities across the country, the hepatitis C program makes use of a comprehensive approach to hepatitis C prevention and treatment that includes screening, testing and counseling, patient and provider education, optimal clinical care, and management of data to continuously improve program quality.
The Hepatitis C Resource Centers (HCRC's), a part of the National Hepatitis C Program, develop best practices in clinical care delivery, patient education, provider education, prevention, and program evaluation that can be used by the entire VA health care system and other medical care systems. They function as field-based clinical laboratories for the development, testing, evaluation, and dissemination of new and innovative products and services for improving the quality of hepatitis C clinical care and education in every VA medical facility.
VA provides extensive information on hepatitis C for health care providers, veterans and their families, and the public at www.hepatitis.va.gov.