|
CDC
Report:
Hepatitis C &
Reused Lancets
Transmission
of
Hepatitis
B Virus
Among
Persons
Undergoing
Blood
Glucose
Monitoring
in
Long-Term--Care
Facilities
---
Mississippi,
North
Carolina,
and Los
Angeles
County,
California,
2003--2004
www.cdc.gov/mmwr/preview/mmwrhtml/mm5409a2.htm
Regular
monitoring
of blood
glucose
levels
is an
important
component
of
routine
diabetes
care
(1).
Capillary
blood is
typically
sampled
with the
use of a
fingerstick
device
and
tested
with a
portable
glucometer.
Because
of
outbreaks
of
hepatitis
B virus
(HBV)
infections
associated
with
glucose
monitoring,
CDC and
the Food
and Drug
Administration
(FDA)
have
recommended
since
1990
that
fingerstick
devices
be
restricted
to
individual
use (2,3).
This
report
describes
three
recent
outbreaks
of HBV
infection
among
residents
in
long-term--care
(LTC)
facilities
that
were
attributed
to
shared
devices
and
other
breaks
in
infection-control
practices
related
to blood
glucose
monitoring.
Findings
from
these
investigations
and
previous
reports
suggest
that
recommendations
concerning
standard
precautions
and the
reuse of
fingerstick
devices
have not
been
adhered
to or
enforced
consistently
in LTC
settings
(2--5).
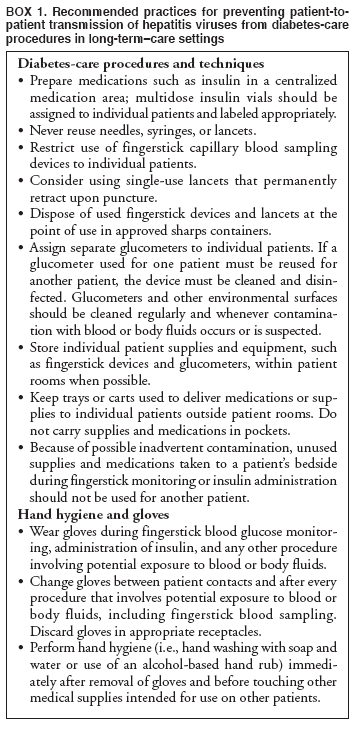
The
findings
underscore
the need
for
education,
training,
adherence
to
standard
precautions,
and
specific
infection-control
recommendations
targeting
diabetes-care
procedures
in LTC
settings
(4--6)
(Box
1).
The
three
outbreaks
described
in this
report
were all
reported
by state
or local
health
departments
to CDC,
which
provided
epidemiologic
and
laboratory
assistance.
In each
of the
three
LTC
settings,
residents
were
tested
for
serologic
markers
for HBV
infection.
Under
the case
definitions
used in
these
investigations,
residents
who
tested
positive
for IgM
antibody
to
hepatitis
B core
antigen
(anti-HBc)
were
defined
as
having
acute
HBV
infection.
Residents
who
tested
positive
for
hepatitis
B
surface
antigen
(HBsAg)
and
total
anti-HBc,
but who
tested
negative
for IgM
anti-HBc,
were
considered
to have
chronic
HBV
infection.
Residents
who
tested
positive
for
total
anti-HBc,
but who
tested
negative
for
HBsAg,
or those
who had
antibody
to HBsAg
(anti-HBs)
>10
milli-International
Units (mIU)
per
milliliter
were
considered
immune
to HBV
infection.
Residents
were
considered
susceptible
to HBV
if they
had no
HBV
markers.
A
retrospective
cohort
study
was
performed
as part
of each
investigation;
the
study
was
restricted
to
acutely
infected
and
susceptible
residents
to
identify
risk
factors.
In all
three
investigations,
staff
members
were
evaluated;
none
were
identified
as
sources
of
infection.
Medical
records
were
reviewed
and
infection-control
procedures
were
assessed
through
direct
observation
and by
interviews
with
nursing
staff
members.
Nursing
Home A,
Mississippi
During
November--December
2003,
the
Mississippi
Department
of
Health
received
reports
of two
fatal
cases of
acute
HBV
infection
among
residents
of
nursing
home A.
The
first
patient
with
recognized
symptoms
of HBV
infection
had
received
serologic
testing
for
viral
hepatitis
infection
in June
2003 as
part of
a
hospital
emergency
department
evaluation
for
abdominal
pain.
Although
this
patient
was
found to
have a
positive
test for
IgM
anti-HBc,
indicating
acute
HBV
infection,
and the
finding
was
noted in
the
patient's
chart in
September
2003,
nursing
home A
did not
contact
the
state
health
department
or
initiate
an
internal
investigation.
Subsequently,
the
patient
died.
In
December
2003,
after a
second
patient
with
acute
HBV
infection
had
died,
and
after a
third
with
acute
HBV
infection
was
reported,
serologic
testing
was
performed
on
specimens
from all
158
residents.
Test
results
were
available
for 160
residents,
including
the two
decedents;
15 (9%)
had
acute
HBV
infection,
one was
chronically
infected,
15 (9%)
were
immune,
and 129
(81%)
were
susceptible.
Percutaneous
and
other
possible
exposures
among
residents
were
evaluated.
Among 38
residents
who
routinely
received
fingersticks
for
glucose
monitoring,
14 had
acute
HBV
infection,
compared
with one
of 106
residents
who did
not
receive
fingersticks
(relative
risk
[RR] =
39.0;
95%
confidence
interval
[CI] =
5.3--290.0).
Glucose
monitoring
of 14
residents
with
acute
HBV
infection
and the
resident
with
chronic
HBV
infection
was
performed
by staff
members
based at
the same
nursing
station.
Reviews
of
infection-control
practices
and site
inspections
indicated
that
each of
the four
nursing
stations
in
nursing
home A
was
equipped
with one
glucometer
and one
spring-loaded,
pen-like
fingerstick
device.
Staff
members
reported
that a
new end
cap and
lancet
assembly
was used
for each
fingerstick
procedure;
however,
the
spring-loaded
barrel
and
glucometer
were not
routinely
cleaned
between
patients.
Investigators
also
observed
that
insulin
and
other
multidose
medication
vials
were not
labeled
with
patient
names or
the
dates
the
vials
were
opened.
In an
anonymous
survey,
several
staff
members
reported
observing
other
workers
reuse a
needle
or
lancet
or fail
to
change
gloves
between
patients.
No other
percutaneous
exposures
were
associated
with
illness.
Assisted
Living
Center
B, Los
Angeles
County,
California
During
January--February
2004,
the Los
Angeles
County
Department
of
Health
Services
received
reports
of four
residents
with
diabetes
in
assisted
living
center B
who had
acute
HBV
infection
during
November
2003--January
2004.
Because
these
initial
reports
were
among
residents
with
diabetes,
serologic
testing
was
performed
in
January
2004 on
residents
who had
received
fingersticks
for
blood
glucose
monitoring
during
May--December
2003. Of
22
residents
tested
(three
declined),
eight
(36%)
had
acute
HBV
infection,
including
the four
residents
previously
identified;
six
(27%)
were
immune
(and
excluded
from the
analysis),
and none
had
chronic
infection.
Reviews
of
patient
records
indicated
that one
of the
acutely
infected
residents
had been
repeatedly
tested
at a
separate
hemodialysis
center
and had
seroconverted
to HBsAg-positive
in July
2003. Of
the nine
patients
who had
daily
exposure
to
fingerstick
procedures
performed
by
nursing
staff,
eight
had
acute
HBV
infection,
compared
with
none
among
the
seven
residents
who
performed
their
own
fingersticks
(RR =
undefined;
CI =
2.8--undefined).
Although
receipt
of
insulin
was also
significantly
associated
with
infection,
two
residents
with
acute
HBV
infection
had not
received
insulin.
Other
percutaneous
exposures
(e.g.,
podiatric
or
dental
care)
were not
associated
with HBV
infection.
Fingerstick
procedures
were
often
performed
by
nursing
staff
members
in a
central
living
area,
with
diabetes
patients
seated
at a
common
table.
Although
residents
had
their
own
fingerstick
devices,
nurses
reported
occasionally
using a
pen-like
fingerstick
device
barrel
from
their
own kits
to
collect
consecutive
blood
samples;
a single
glucometer
was
typically
used for
all
residents.
Nurses
reported
that
they
were
discouraged
from
wearing
gloves
to
decrease
the
sense of
a
clinical
environment,
and hand
hygiene
was not
performed
between
procedures.
Nursing
Home C,
North
Carolina
In
May
2003, a
case of
HBV
infection
in a
resident
of
nursing
home C
was
reported
to the
North
Carolina
Department
of
Health.
During
June--July
2003,
serologic
testing
was
performed
on
specimens
from all
192
residents;
11 (6%)
had
acute
HBV
infection,
16 (8%)
were
immune,
and 165
(86%)
were
susceptible.
No
resident
had
chronic
HBV
infection.
Of 45
residents
who
received
fingersticks
for
glucose
monitoring,
eight
(18%)
had
acute
HBV
infection,
compared
with
three
(3%) of
117
residents
without
this
exposure
(RR =
6.9; CI
=
1.9--25.0).
After
data
were
controlled
for
fingerstick
exposures,
acute
HBV
infection
was not
associated
with
other
percutaneous
exposures
(e.g.,
insulin
injections,
podiatry
procedures,
or
phlebotomy).
Two
diabetes
patients
at
nursing
home C
who were
potential
sources
of the
outbreak
were
identified
retrospectively;
one had
clinical
symptoms
of
hepatitis
B and
serologic
markers
of acute
infection
during
2002,
whereas
the
other
had
chronic
HBV
infection
and died
in
February
2002.
Interviews
with
staff
and
direct
observation
of
glucose-monitoring
practices
revealed
that
only
single-use
lancets
were
used,
and
insulin
vials
were not
shared
among
patients.
However,
on each
wing of
the
facility,
a single
glucometer
was used
for all
patients
receiving
fingersticks;
glucometers
were not
routinely
cleaned
between
patients.
On some
days, a
single
health-care
worker
performed
approximately
20
fingerstick
procedures
during a
single
work
shift.
In an
anonymous
survey,
nursing
staff
members
indicated
that
some
health-care
workers
did not
always
change
gloves
between
patients
when
performing
fingerstick
procedures.
Reported
by: R
Webb,
MD, M
Currier,
MD, J
Weir, KM
McNeill,
MD,
Mississippi
Dept of
Health.
E
Bancroft,
MD, D
Dassey,
MD, J
Maynard,
D
Terashita,
MD, Los
Angeles
County
Dept of
Health
Svcs,
California.
K
Simeonsson,
MD, A
Chelminski,
J Engel,
MD,
North
Carolina
Dept of
Health
and
Human
Svcs. JF
Perz,
DrPH, AE
Fiore,
MD, IT
Williams,
PhD, BP
Bell,
MD, Div
of Viral
Hepatitis,
National
Center
for
Infectious
Diseases;
T
Harrington,
MD, C
Wheeler,
MD, EIS
officers,
CDC.
Editorial
Note:
Lack
of
adherence
to
standard
precautions
and
failure
to
implement
long-standing
recommendations
against
sharing
fingerstick
devices
place
LTC
residents
at risk
for
acquiring
infections
from
bloodborne
pathogens
such as
HBV (2,3,7).
In
nursing
home A,
the
spring-loaded
barrel
of a
fingerstick
device
was used
for
multiple
patients.
Previous
outbreaks
have
been
linked
to such
devices
when the
platform
or
barrel
supporting
the
disposable
lancet
was
reused
for
multiple
patients,
when
used
lancets
were
stored
with
unused
lancets,
or when
lancet
caps
were
reused (2,3;
CDC,
unpublished
data,
1999).
In
assisted
living
center
B,
nursing
staff
members
routinely
administered
fingersticks
without
wearing
gloves
or
performing
hand
hygiene
between
patients,
and
spring-loaded
fingerstick
devices
were
also
occasionally
shared.
In
nursing
home C,
as with
other
recent
outbreaks
(8; CDC,
unpublished
data,
2002),
transmission
of HBV
among
residents
with
diabetes
occurred
despite
use of
single-use
fingerstick
devices
or
insulin
medication
vials
that
were
dedicated
for
individual
patient
use. In
these
settings,
glucose
monitors,
insulin
vials,
or other
surfaces
contaminated
with
blood
from an
HBV-infected
person
might
have
resulted
in
transfer
of
infectious
virus to
a
health-care
worker's
gloves
and to
the
fingerstick
wound or
subcutaneous
injection
site of
a
susceptible
resident.
Similar
indirect
transmission
of HBV
in
health-care
settings
through
contaminated
environmental
surfaces
or
inadequately
disinfected
equipment
has been
reported
with
other
health-care
procedures,
such as
dialysis
(6,9).
HBV is
stable
at
ambient
temperatures;
infected
patients,
who
often
lack
clinical
symptoms
of
hepatitis,
can have
high
concentrations
of HBV
in their
blood or
body
fluids
(6). To
prevent
patient-to-patient
transmission
of
infections
through
cross-contamination,
health-care
providers
should
avoid
carrying
supplies
from
resident
to
resident
and
avoid
sharing
devices,
including
glucometers,
among
residents.
The
risk for
patient-to-patient
transmission
of HBV
infection
can be
reduced
by
implementing
specific
prevention
measures
(Boxes
1
and
2).
LTC
staff
often
perform
numerous
percutaneous
procedures;
frequent
blood
glucose
monitoring
increases
opportunities
for
bloodborne
pathogen
transmission.
The
outbreak
investigations
reported
here
identified
residents
with
diabetes
who
received
fingersticks
from
nursing
staff
members
as often
as four
times
per day,
according
to their
physician's
routine
orders,
despite
having
consistently
normal
glucose
levels.
Expert
panels
have
concluded
that
approximately
8 years
are
needed
before
the
benefits
of
glycemic
control
result
in
reductions
in
microvascular
complications
(1,10).
In LTC
settings,
schedules
for
fingerstick
blood
sampling
of
individual
patients
should
be
reviewed
regularly
to
reduce
the
number
of
percutaneous
procedures
to the
minimum
necessary
for
their
appropriate
medical
management.
In each
of the
investigations
described
in this
report,
implementation
of
infection-control
measures
(Boxes
1
and
2)
was
recommended,
along
with
follow-up
serologic
testing
for
markers
of HBV.
An
estimated
70,000--80,000
HBV
infections
occur
each
year in
the
United
States.
Most of
these
infections
occur
among
young
adults
with
behavioral
risk
factors
(i.e.,
sexual
contact
and
injection-drug
use);
these
adults
should
receive
hepatitis
B
vaccine.
Preventing
transmission
of HBV
among
patients
in
long-term--care
settings
requires
adherence
to
recommended
infection-control
practices
and
prompt
response
to
identified
instances
of
transmission.
Routine
hepatitis
B
vaccination
or
screening
of LTC
residents
is not
recommended.
In the
outbreaks
described
in this
report,
initial
cases
were not
identified
or
investigated
in a
timely
fashion,
resulting
in
missed
opportunities
to
correct
deficient
practices
and
interrupt
transmission.
Evidence
of acute
viral
hepatitis
in any
LTC
resident
should
prompt a
thorough
investigation.
For a
case
involving
a
resident
with
diabetes,
fingerstick
blood
sampling
procedures
and
insulin
administration
should
receive
particular
scrutiny.
Health
departments
should
encourage
reporting
of such
cases
and
offer
assistance
in
identifying
the
source
of
infection.
CDC
continues
to
support
investigations
in LTC
and
other
health-care
settings
and is
working
toward
improved
implementation
of the
infection-control
recommendations
described
in this
report.
Acknowledgments
The
findings
in this
report
are
based,
in part,
on data
provided
by C
Ranck, R
Hotchkiss,
B Amy,
MD,
Mississippi
Dept of
Health.
J
Rosenberg,
MD, Div
of
Communicable
Disease
Control,
California
Dept of
Health
Svcs. P
MacDonald,
PhD,
Dept of
Epidemiology,
Univ of
North
Carolina,
Chapel
Hill; S
Smith, P
Poole,
North
Carolina
Dept of
Health
and
Human
Svcs. M
Viray,
Epidemiology
Program
Office,
CDC.
References
-
American
Diabetes
Association.
Standards
of
medical
care
in
diabetes.
Diabetes
Care
2004;27:S15--35.
-
CDC.
Nosocomial
transmission
of
hepatitis
B
virus
associated
with
a
spring-loaded
fingerstick
device---California.
MMWR
1990;39:610--3.
-
CDC.
Nosocomial
hepatitis
B
virus
infection
associated
with
reusable
fingerstick
blood
sampling
devices---Ohio
and
New
York
City,
1996.
MMWR
1997;46:217--21.
-
CDC.
Update:
universal
precautions
for
prevention
of
transmission
of
human
immunodeficiency
virus,
hepatitis
B
virus,
and
other
bloodborne
pathogens
in
health-care
settings.
MMWR
1988;37:377--88.
-
American
Association
of
Diabetes
Educators.
Educating
providers
and
persons
with
diabetes
to
prevent
the
transmission
of
bloodborne
infections
and
avoid
injuries
from
sharps.
Chicago,
IL:
American
Association
of
Diabetes
Educators;
1997.
Available
at
http://www.aadenet.org/PublicAffairs/PositionStatements/EducProvidersBloodborneInfetions.pdf.
-
Williams
IT,
Perz
JF,
Bell
BP.
Viral
hepatitis
transmission
in
ambulatory
health
care
settings.
Clin
Infect
Dis
2004;38:1592--8.
-
Desenclos
JC,
Bourdiol-Razes
M,
Rolin
B,
et
al.
Hepatitis
C in
a
ward
for
cystic
fibrosis
and
diabetic
patients:
possible
transmission
by
spring-loaded
finger-stick
devices
for
self-monitoring
of
capillary
blood
glucose.
Infect
Control
Hosp
Epidemiol
2001;22:701--7.
-
Khan
AJ,
Cotter
SM,
Schulz
B,
et
al.
Nosocomial
transmission
of
hepatitis
B
virus
infection
among
residents
with
diabetes
in a
skilled
nursing
facility.
Infect
Control
Hosp
Epidemiol
2002;23:313--8.
-
CDC.
Recommendations
for
preventing
transmission
of
infections
among
chronic
hemodialysis
patients.
MMWR
2001;50(No.
RR-5).
-
Brown
AF,
Mangione
CM,
Saliba
D,
Sarkisian
CA;
California
Healthcare
Foundation/American
Geriatrics
Society
Panel
on
Improving
Care
for
Elders
with
Diabetes.
Guidelines
for
improving
the
care
of
the
older
person
with
diabetes
mellitus.
J Am
Geriatr
Soc
2003;51:
S265--80.
Recommended
practices
for
preventing
patient-to-patient
transmission
of
hepatitis
viruses.
During
service
providers
didn't
wear
gloves,
and
reused
the
lancet.
|