|
Watch video
Manufacturer
takes credit for
eradicating
small pox but
fails to mention
the injections
were
contaminated.
More info:
2002 Small Pox
Needles & Jet
Injectors
THE SMALLPOX
VACCINE
Is the use of a
jet injector gun
the best way to
administer the
vaccination?
Around 1972
Military began
to administer
the small pox
vaccine with a
bifurcated
needle on all
recruits and
booster shots
administered in
the field, which
proved a greater
risk of
transmitting
disease due to
the fact the
same vial and
needle was
reused.
November 2002THE
SMALLPOX VACCINE
David Snodgrass of Tucson, AZ asks:
Is the use of a jet injector gun the best way to administer the
vaccination? In 1967, if memory serves, that was the method used to give
me the vaccine.
Medical epidemiologist Dr. Lisa Rotz responds:
___________________________
The vaccine formulations now available are not formulated for the jet
injector gun. Current day problems [with jet injector guns] include
concerns about transmission of other infectious diseases such as hepatitis
(there have been some outbreaks). The smallpox vaccine is not given with a
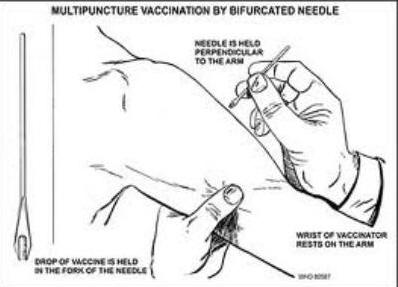
hypodermic needle. It is not a "shot," like many vaccinations. The vaccine
is given using a bifurcated (two-pronged) needle that is dipped into the
vaccine solution. When removed, the needle retains a droplet of the
vaccine. The needle is then used to quickly prick the skin 15 times in a
few seconds. The pricking is not deep, but it will cause a sore spot and
one or two drops of blood to form. The vaccine usually is given in the
upper arm.
If the vaccination is successful, a red and itchy bump develops at the
vaccination site in three or four days. In the first week after
vaccination, the bump becomes a large blister, fills with pus, and begins
to drain. During week two, the blister begins to dry up and a scab forms.
The scab falls off in the third week, leaving a small scar. People who are
being vaccinated for the first time may have a stronger "take" (a
successful reaction) than those who are being revaccinated.
http://www.pbs.org/newshour/health/bioterrorism/forum.html. |
The Study:
J Clin Gastroenterol. 2005
Mar;39(3):243-6.
Association between smallpox
vaccination and hepatitis C antibody
positive serology in Pakistani
volunteers.
Aslam M, Aslam J, Mitchell BD, Munir
KM.
Source
Punjab Hepatitis Research Center,
31/10A Abu Bakr Block, New
Gardentown, Lahore, Pakistan.
Abstract
GOALS:
To determine whether the smallpox
vaccination program has
significantly contributed to the
widespread prevalence of hepatitis C
infection in Pakistan.
BACKGROUND:
Hepatitis C virus has become a
worldwide pandemic and has
especially devastated developing
nations such as Pakistan. There
continues to be an increase in
fatalities due to hepatitis
C-related cirrhosis in Pakistan.
STUDY:
We studied 523 volunteers in the
city of Lahore to determine whether
the smallpox vaccination program,
which ran from 1964 to 1982 in
Pakistan, may be responsible for the
national surge in hepatitis C viral
infection, perhaps because of
repetitive use of vaccination
devices without proper sterilization
or to contaminated vaccine contents.
RESULTS:
There was a significantly higher
likelihood of hepatitis C antibody
seroprevalence in individuals
vaccinated for smallpox versus
nonvaccinated individuals (21.0% vs.
4.6%, P < 0.001, age-adjusted
odds ratio, 3.39; 95% confidence
interval, 1.36-8.46). Subjects with
positive hepatitis C serology were
also more likely to have a history
of transfusions (19.2% vs. 9.0%, P =
0.01), but anti-HCV positive
serology was not significantly
associated with a history of surgery
or dental procedures. Following
adjustment for age, sex, and history
of other conditions, including
transfusion, the association between
prior smallpox vaccination and
hepatitis C antibody seroprevalence
remained strong and highly
significant (multivariate adjusted
odds ratio, 6.11; 95% confidence
interval, 2.58-14.51).
CONCLUSION:
These results suggest that the
widespread prevalence of hepatitis C
infection in Pakistan may be an
unintended consequence of the
country's smallpox vaccination
program and that blood transfusion
is also a significant risk factor.
________________________________________________________________
Corroborating Evidence: By Shaun
Brown
I came across a post from a lady
named Cindy who questioned and
researched the possibility of HCV
being transmitted from smallpox
vaccinations. Reading through the
thread I was utterly surprised to
learn that several years later Cindy
had developed liver cancer and had
passed away. As you know, having
lost my father from hepatitis C from
the jet injector this stirred up
some emotions within me. I felt
compelled to further bring to light
Cindy’s findings. Cindy had
disclosed the above study conducted
in Pakistan that found an
association between individuals with
HCV and the smallpox vaccination
campaign. Along with corroborating
evidence from other sources,
demonstrate the jet injector and
bifurcated needle transmitted
hepatitis C in a specific area of
Pakistan. Certainly Cindy deserves
the recognition for this find.
In 1988, Fenner and colleagues, in
conjunction with the World Health
Organization, published Smallpox
and Its Eradication (the
attached document lists links to
each chapter). The following facts
each support the premise that jet
injectors and bifurcated needles
were widely used within Pakistan’s
smallpox eradication program.
Fact: Prior to 1967, the vaccination
methods commonly used for
administering smallpox vaccination
were scarification, multiple
pressure method, and the rotary
lancet. The rotary lancet was
disapproved of by WHO. Staff amongst
the smallpox campaign in Pakistan
often confiscated the rotary
lancets, opting for newer
vaccination technologies. (chapter
7, pgs 292 - 293)
“ Although the WHO Expert Committee
on Smallpox (1964) recommended that
this method [rotary lancet] should
not be used, it was still routinely
employed in some parts of the Indian
subcontinent long after this. During
the smallpox eradication programmes
in Pakistan and India (see Chapters
14 and 15), the programme staff
hunted for rotary lancets and
confiscated a large number of them
from vaccinators who were reluctant
to abandon the method but were thus
obliged to use the bifurcated
needle.” (chapter 7, pg 293)
Fact: “WHO provided some l00 jet
injectors to the national programmes
in Pakistan, the Sudan and Zaire in
1967 and 1968.” (chapter 11, pg 578)
Fact: “Jet injectors (trade name Ped-o-Jet)
played an important role during the
initial phase of the Intensified
Smallpox Eradication Programme. They
were used to ensure rapid
vaccination coverage with
satisfactory take rates in national
smallpox eradication programmes in
Brazil, Zaire, countries in western
and central Africa, and to a small
extent in several other countries.”
(chapter 11, pg 573)
Fact: In 1967, the Pakistan smallpox
vaccination campaign administered
22,681,000 vaccinations. (chapter
14, pg 686, Table 14.18)
Fact: In 1968, this same campaign
administered 13,946,000 vaccinations
(chapter 14, pg 686, Table 14.18)
Fact: From 1969 to 1970, a mass
vaccination campaign was conducted
in the Punjab Province of Pakistan,
in which 25,600,000 smallpox
vaccinations were administered.
(chapter 14, pg 693).
Fact: The city of Lahore resides
within the Punjab Province.
Fact: By 1971, “In Lahore, 93% of
all persons surveyed showed
vaccination scars or the pockmarks
of smallpox. Even among infants
under 1 year of age 39% were
protected, and among children aged
1-4 years 84% were protected
(WHO/SE/69.13, Heiner et al.; Ali &
Heiner, 1971).” (chapter 14, pg 689)
Fact: “…vaccination by the jet
injector sometimes resulted in a
very small scar which might be
overlooked on the skin of subjects
bearing many scars of traumatic
origin. In spite of these
shortcomings, the vaccination scar
provided a more easily determined
and reliable index of an
individual's immune status vis-a-vis
smallpox than was possible with
other infectious diseases.” (chapter
1, pg 5).
Fact: “A few disadvantages of jet
injectors emerged during the
campaigns in which they were used.
In contrast to the simplicity of
bifurcated needles, the jet injector
required meticulous care and
maintenance and considerable repair
skills, which could not always be
provided despite all the efforts to
prepare a detailed, profusely
illustrated manual.” (chapter 11, pg
579)
Fact: “Vaccinators were advised to
use the multiple puncture method
with the bifurcated needle with
enough force to cause slight
bleeding.” (chapter 11, pg 569)
Fact: “Detailed instructions
(SEl68.2 Rev.1) were widely
circulated and it was pointed out in
them that, with the multiple
puncture method, a trace of blood
indicated that the punctures were
likely to have introduced the virus
into the epidermis.” (chapter 11, pg
572)
Fact: “…early in 1968, the Smallpox
Eradication unit sought a plastic
container which would hold about 100
needles, would be cheap replica watches brands to produce
and could be sterilized by boiling.
The containers eventually used were
designed by Dr Shafa, who was
successful in stimulating local
producers in Bangladesh and Pakistan
to produce the top replica watches container illustrated
in Plate 11.1 5. After the conical
end had been unscrewed, needles were
placed in the knockoff watches containers with the
prongs towards the base, and were
sterilized by placing the closed
container in boiling water. The
bottom of the container was provided
with a few holes so that the water
could be drained or shaken off after
boiling. In the field, needles could
be removed aseptically from the
container one at a time through the
hole at the apex of the conical lid,
and placed in an empty container
after use, for sterilization next
day.” (chapter 11, pg 572)
Was boiling medical instruments in
water for “X” amount of time
sufficient to kill the hepatitis C
virus?
Inference: In spite of the emergence
of the more simple and practical
bifurcated needle in 1969, and the
mass vaccination campaign in Punjab
province from 1969 to 1970, it can
be inferred from 1969 to 1970 jet
injectors were still used in some
cases as evidenced of “vaccination
scars” in Lahore in 1971. Whereupon
WHO attributes “vaccination scars”
for this period as resulting from
jet injectors and pockmarks
resulting from bifurcated needles.
Rotary lancets also produced
vaccination scars, with the scar
being slightly larger than that of
jet injectors. Although, the rotary
lancet was being decommissioned and
often confiscated by WHO staff.
Therefore, it’s use was unlikely
after 1967.
The following facts along with
Aslam’s 2005 multivariate study
provide evidence to Weniger’s 2008
paper (The Unintended Consequences
of Vaccine Delivery Devices Used to
Eradicate Smallpox: Lessons for
Evaluating Future Vaccination
Methods) which highlighted the
theoretical risk of blood-borne
disease transmission from MUNJI and
bifurcated needles used during the
smallpox eradication campaign.2008
Jet injectors & Bifurcated Needles
________________________________________________________________
Ex Cetera…
In my research I found old
government videos that show the Ped-O-Jet
used in a smallpox vaccination
campaign in Tonga, and a measles
vaccination campaign in Africa.
These videos both show the jet
injector used consecutively from
patient-to-patient without the
nozzle being wiped or cleaned.
Miracle In Tonga
http://collections.nlm.nih.gov/catalog/nlm:nlmuid-7800975A-vid
Mission, measles: the story of a
vaccine
http://collections.nlm.nih.gov/catalog/nlm:nlmuid-8901910A-vid
 |




